-
8/14/2019 Enfermedad Cardiovascular Materna
1/12
DOI: 10.1542/neo.13-11-e6512012;13;e651 Neoreviews
Alexandria J. Hill and Luis D. PachecoCardiovascular Disease in
Pregnancy
http://neoreviews.aappublications.org/content/13/11/e651located
on the World Wide Web at:
The online version of this article, along with updated
information and services, is
ISSN: .60007. Copyright 2012 by the American Academy of
Pediatrics. All rights reserved. Printthe American Academy of
Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village,
Illinois,it has been published continuously since . Neoreviews is
owned, published, and trademarked byNeoreviews is the official
journal of the American Academy of Pediatrics. A monthly
publication,
at Health Internetwork on January 27,
2013http://neoreviews.aappublications.org/ Downloaded from
http://http//neoreviews.aappublications.org/content/13/11/e651http://http//neoreviews.aappublications.org/content/13/11/e651http://http//neoreviews.aappublications.org/content/13/11/e651http://neoreviews.aappublications.org/http://neoreviews.aappublications.org/http://neoreviews.aappublications.org/http://neoreviews.aappublications.org/http://http//neoreviews.aappublications.org/content/13/11/e651
-
8/14/2019 Enfermedad Cardiovascular Materna
2/12
Cardiovascular Disease in PregnancyAlexandria J. Hill, MD,Luis
D. Pacheco, MD
Author DisclosureDrs Hill and Pachecohave disclosed nonancial
relationshipsrelevant to this article.This commentary doescontain a
discussion of an unapproved/investigative use of a commercial
product/device.
Educational GapsFetuses and newborns of mothers with
cardiovascular disease face a range of risks relatedto the type of
maternal disease, the drugs used to manage it, and the
inheritability of thedisease.
Abstract Although cardiac lesions in pregnancy are often well
tolerated, those that are not war-rant a cardiac evaluation as well
as careful management in the antepartum and peripar-tum periods.
Congenital heart disease cases comprise the majority of pregnant
cardiacpatients, and the lesions can require careful monitoring.
Women who have valvulardisease often tolerate pregnancy well, but
there are speci c lesions that require closemonitoring throughout
the pregnancy. Finally, peripartum cardiomyopathy, althoughrare, is
of great concern and must be managed quickly and appropriately. We
will re- view concerns and treatment for pregnant women who have
congenital heart disease, valvular lesions, and peripartum
cardiomyopathy, as well as provide guidance for drugtherapy in the
pregnant patient who has cardiac disease.
Objectives After completing this article, readers should be able
to:1. Identify common congenital heart lesions seen in the pregnant
patient and
understand basic management for each lesion.2. Understand
medical management for valvular cardiac disease in pregnancy.3.
Classify heart lesions according to patient symptoms.
4. List medications that should not be used for cardiac patients
in pregnancy.
IntroductionCardiac disease in the pregnantpatient is
encountered more andmore often because of womensurviving prior
cardiac surgeries as well as the advances in assisted reproductive
medicine. Infact, more than one half of cardiac patients managed
obstetrically have congenital heart disease(CHD). Currently, the
incidence of cardiac disease in pregnancy is w 4% but notably the
mor-bidity can be much higher (34%). The leading causes for
maternal mortality consist of cardio-myopathy, pulmonary
hypertension, aortic dissection, and myocardial infarction.
Many physiologic changes occur in the pregnant patient (Table
1). Although total body volume increases, red bloodcell volume
increases at a lower rate, causing a dilutional ane-
mia. This anemia allows the pregnant woman to have less viscous
blood to better perfuse her placenta to nurturethe fetus. The heart
compensates for the overall increased volume during pregnancy with
decreased blood pressure(nadir at the late second to early third
trimester) and de-creased systemic vascular resistance (SVR).
Moreover,the cardiac output is greatly increased, starting as early
as8 weeks gestation.
Patients who have cardiac disease in pregnancy shouldbe classi
ed according to any limitations in their physical
AbbreviationsAS: aortic stenosisASD: atrial septal defect CHD:
congenital heart diseaseNYHA: New York Heart AssociationPDA: patent
ductus arteriosusPVR: pulmonary vascular resistanceSVR: systemic
vascular resistanceUFH: unfractionated heparin VSD: ventricular
septal defect
Department of MaternalFetal Medicine, University of Texas
Medical Branch, Galveston, TX.
Article maternal-fetal medicine
NeoReviews Vol.13 No.11 November 2012 e651
at Health Internetwork on January 27,
2013http://neoreviews.aappublications.org/ Downloaded from
http://neoreviews.aappublications.org/http://neoreviews.aappublications.org/http://neoreviews.aappublications.org/http://neoreviews.aappublications.org/
-
8/14/2019 Enfermedad Cardiovascular Materna
3/12
activity as well as symptoms they experience at rest or with
physical activity. The basic criteria for the New York
Heart Association (NYHA) classi cation system can befound in
Fig1. This classi cation system may beused in pre-conceptional
counseling for patients who have known car-diac disease. We will
address patients who have cardiacdisease encountered in
theobstetric world, including those who have CHD, valvular disease,
and cardiomyopathy, as well as discuss medications used in
pregnancy.
Congenital Heart DiseaseCHD is the most common form of heart
disease man-aged in pregnancy. Generally, the pregnant patient who
has CHD should avoid uid overload and be placedin the left lateral
decubitus position when laboring. Thepatient should be provided
oxygen during labor, and theuse of epidural anesthesia should be
evaluated by the an-esthesiology service. In general, narcotic
epidurals arepermissible for these patients. Management
principlesfor CHD are listed in Table 2. Routine thromboembo-lism
prophylaxis is not administered for any of the
CHD lesions but should be strongly considered for pa-tients who
have Eisenmenger syndrome because they have a higher rate of
thromboembolism. Each lesion isdiscussed brie y in the following
text.
Patent Ductus Arteriosus Although patent ductus arteriosus (PDA)
is common inthe neonate, surgery is often performed early in age;
thus,this lesion is not often encountered in pregnancy. A re-paired
PDA is well tolerated in pregnancy. However, if a large PDA is
present, pulmonary hypertension and ulti-mately Eisenmenger
syndrome are possible complications.
Atrial Septal Defect An atrial septal defect (ASD) is the most
common lesionencountered in the pregnant patient. These defectsare
generally well tolerated in pregnancy and, even if un-repaired,
rarely cause complications. If the defect islarge, shunt reversal
and/or cardiac arrhythmias may oc-cur. Any reversal to a
right-to-left shunt should causeconcern for pulmonary hypertension
and Eisenmengersyndrome.
Ventricular Septal DefectEven thoughventricular septal defect
(VSD) is a commonlesion in the neonatal population, it is rarely
seen in the
pregnant patient because most VSDs close in the rst few years
after birth or are repaired in childhood. Regardless if the lesion
is repaired or unrepaired, an echocardiogram is warranted in
pregnancy. If the VSD is patent, blood most often ows from left to
right. If there is concern for right ventricular hypertrophy,
reversal of a patent shunt ishighly possible, and the possibility
of Eisenmenger syn-drome must be considered.
Coarctation of the AortaPatients who have coarctation may often
have co-existingcardiac defects such as septal defects or a
bicuspid aortic
valve. Patients undergo repair when there is a signi cant
difference in pressure gradients between the upper andlower
extremities. These patients are also at a higher risk of
intracranial aneurysms. Therefore, rupture of the aortaas well as
potential intracranial aneurysms are possibleconcerns. If the
coarctation is signi cant, the mother isat higher risk of
hypertension; overall, these patientscarry a higher risk of
pre-eclampsia. Stable patients canundergo vaginal delivery, but use
of the Valsalva maneu- ver during the second stage of labor should
be mini-mized. Patients who have coarctation of the aortashould
maintain an adequate preload and avoid hypoten-sion (Table 2).
Table 1. Physiologic Changes inPregnancy
Physiologic Change % Change
Heart rate [ 1020Stroke volume [ 30Cardiac output [ 3050Blood
volume [ 2050Systemic vascular resistance Y 20
Figure 1. New York Heart Association (NYHA)
functionalclassication.
maternal-fetal medicine cardiovascular
e652 NeoReviews Vol.13 No.11 November 2012
at Health Internetwork on January 27,
2013http://neoreviews.aappublications.org/ Downloaded from
http://neoreviews.aappublications.org/http://neoreviews.aappublications.org/http://neoreviews.aappublications.org/http://neoreviews.aappublications.org/
-
8/14/2019 Enfermedad Cardiovascular Materna
4/12
Tetralogy of FallotThe tetrad of VSD, overriding aorta, right
ventricularhypertrophy, and pulmonary stenosis often has
beencorrected surgically by the time a patient reaches
child-bearing age and thus is well tolerated in pregnancy. These
women should be monitored for pulmonary regurgita-tion because it
places them at the greatest risk forcomplications such as
arrhythmia and heart failure. Echo-cardiograms should be performed
on these women to as-sess for any remaining cardiac shunts that
could placethem at increased risk for pulmonary hypertension.
Eisenmenger SyndromeThis syndrome occurs when a left-to-right
intracardiacshunt (PDA, ASD, or VSD) shifts to a right-to-left
shunt.This happens when the pulmonary vasculature system
isoverloaded, resulting in pulmonary hypertension, whichprovides
enough pressure to reverse the shunt. In severecases, a heart lung
transplant may be the ultimate
treatment for this diagnosis. SVR decreases in pregnancy.If a
woman experiences hypertension, she will have an in-crease in SVR,
which could then lead to a worsening of a left-to-right shunt.
Equally, if the pulmonary vascularresistance (PVR) falls, a
left-to-right shunt can worsen.Therefore, increases in SVR and
decreases in PVR shouldbe avoided in patients who have a PDA, ASD,
or VSD. When a patient has already experienced reversal of a shunt,
and thus has a right-to-left shunt with pulmonary hypertension, it
is important to avoid increases in PVR (metabolic acidosis,
hypoxia, or lung hyperin ation), which could worsen a right-to-left
shunt.
Marfan SyndromeMarfan syndrome is an autosomal dominant
conditionthat will be accompanied by cardiac complications 80%of
the time. The main concern is a dilation of the aorticroot and
therefore risk of dissection or rupture. It isrecommended that
women undergo repair before
Table 2. Management of Congenital Heart Disease in
PregnancyCardiac Lesion Medical Management
Patent ductus arteriosus Avoid: hypertension, a decrease in
PVR,a arrhythmias, tachycardia a,b
Atrial septal defect Avoid: hypertension, a decrease in PVR,a
arrhythmias, tachycardia a,b
Ventricular septal defect Avoid: hypertension, a decrease in
PVR,a arrhythmias, tachycardia a,b
Coarctation Avoid: hypotension, bradycardia, myocardial
depressants, excess blood lossTetralogy of Fallotc Avoid:
hypotension, bradycardia, myocardial depressants, excess blood
lossEisenmenger syndromec Avoid: hypotension, excess blood loss,
increase in PVR, myocardial depressants
Treatment: CCB, inotropic agents, diuretics, oxygen,
anticoagulationMarfan syndrome Avoid: hypertension, tachycardia,
positive inotropic drugs
Treatment: b -blockers (keep HR< 90 beats per minute when at
rest)
CCB calcium channel blocker; HR heart rate; PVR pulmonary
vascular resistance.a Can lead to increase in left-to-right shunt.b
If pulmonary hypertension is present, avoid increase in PVR (ie,
hypoxemia, nitrous oxide, hypercarbia, vasoconstrictors) because it
can worsen a right-to-left
shunt.c No epidural; may consider with Tetraology of Fallot if
no intracardiac shunt is present.
Table 3. Recurrence Risk of Fetal Congenital Heart Defects in
FutureFetus (%)
Cardiac Lesion Prior Affected Sibling Father Affected Mother
Affected
Tetralogy of Fallot 2.5 1.5 2.6Aortic coarctation 14.1Atrial
septal defect 2.5 1.5 4.611 Ventricular septal defect 3 2
9.515.6Pulmonary stenosis 2 2 6.5Aortic stenosis 2 3 1517.9Patent
ductus arteriosus 3 2.5 4.1Marfan syndrome 50 50
maternal-fetal medicine cardiovascular
NeoReviews Vol.13 No.11 November 2012 e653
at Health Internetwork on January 27,
2013http://neoreviews.aappublications.org/ Downloaded from
http://neoreviews.aappublications.org/http://neoreviews.aappublications.org/http://neoreviews.aappublications.org/http://neoreviews.aappublications.org/
-
8/14/2019 Enfermedad Cardiovascular Materna
5/12
pregnancy if the dilation of the aortais more than 4.5 cm. Risk
of rupture when the aorta is not dilated is ex-tremely low ( <
1%). In labor, women should be encouraged tominimize the use of the
Valsalvamaneuver. Women should be coun-seled strongly regarding the
highrisk of having a neonate who hasMarfan syndrome (Table 3).
Ebstein AnomalyEbstein anomaly is rarely seen in thepregnant
population, and reportedcases resulted in no maternal
compli-cations and neonatal complicationsof prematurity and
congenital car-diac abnormalities. This anomaly isde ned as apical
displacement of the tricuspid septal lea et and is al- ways
accompanied by tricuspid re-gurgitation, which can lead to right
atrial dilation. Onehalf of these patients have a co-existing ASD
or PDA.
Transposition of the Great VesselsPatients who have complete
transposition of the great ves-sels whoreach childbearing age have
undergone correctiveprocedures, most commonly an atrial switch
(Mustardprocedure). These women tolerate pregnancy well but can
eventually experience irreversible right
ventriculardysfunction.
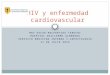
Finally, when counseling a mother who has CHD, sheshould be
aware that she has approximately a 5% chance of having a child who
has CHD. Also, the mother should be
counseled on the risk of recurrence of CHD in the fetusdepending
on the type of maternal CHD (Table 3). Mater-nal mortality risks
should also be reviewed and can vary widely, from less than 1% with
ASD and VSD up to 25%to 50% in patients who have pulmonary
hypertension
(Fig 2).
Valvular Heart Disease Valvular lesions are either congenital or
acquired, andmost lesions seen in pregnancy are acquired from
rheu-matic fever. Of the valves affected, the mitral valve isthe
most common, followed by the aortic, tricuspid,and then pulmonic
valves. Women who present with
Figure 2. Maternal mortality associated with cardiac lesions in
pregnancy. AS [ aorticstenosis; ASD[ atrial septal defect; PDA[
patent ductus arteriosus; MI [ myocardialinfarction; MS [ mitral
stenosis; NYHA[ New York Heart Association; VSD[ ventricularseptal
defect.
Table 4. Classication of Valvular Heart Lesions According to
Maternal
and Fetal RisksLow Maternal and/or Fetal Risks High Maternal
and/or Fetal Risks
Asymptomatic AS with low mean outow gradient andnormal LV
systolic function (EF > 50%)
Severe AS with or without symptoms
NYHA I or II AR and normal LV systolic function NYHA IIIIV and
AR (or MR)NYHA I or II MR and normal LV systolic function NYHA IIIV
and MSMVP with no MR (if mild to moderate MR and normal LV
systolic function)Aortic and/or mitral disease with severe
pulmonary
hypertension or LV systolic dysfunction (EF < 40%)Mild MS
without pulmonary hypertension Marfan syndrome with or without
ARMild to moderate pulmonary stenosis Mechanical prosthetic valve
requiring anticoagulation
AR aortic regurgitation; AS aortic stenosis; EF ejection
fraction; LV left ventricular; MR mitral regurgitation; MS mitral
stenosis; NYHA New York Heart Association.
maternal-fetal medicine cardiovascular
e654 NeoReviews Vol.13 No.11 November 2012
at Health Internetwork on January 27,
2013http://neoreviews.aappublications.org/ Downloaded from
http://neoreviews.aappublications.org/http://neoreviews.aappublications.org/http://neoreviews.aappublications.org/http://neoreviews.aappublications.org/
-
8/14/2019 Enfermedad Cardiovascular Materna
6/12
a valvular lesion in pregnancy should be counseled regard-ing
their risks during the pregnancy. After identifying thelesionand
the NYHA classi cation, onecan further classify the patient into
low or high maternal and/or fetal risks(Table 4). NYHA I patients
fall into the low-risk cat-egory. Conversely, patients who fall
into NYHA III orIV carry higher risks during pregnancy.
Patients who have tricuspid lesions usually have an iso-lated
lesion, which is well tolerated during pregnancy. Re-gurgitant
lesions in the mitral and aortic valves, mitralvalveprolapse, and
pulmonary stenosis also cause minimal con-cern in thepregnant
patient. Moreover, these lesions rarely require treatment
throughout pregnancy or during labor.Stenotic lesions of the mitral
and aortic valveare most con-cerning in pregnancy and will be
addressed speci cally inthis section. General management criteria
for patients whohave valvular disease in pregnancy can be found in
Table 5.
Mitral StenosisMitral stenosis is the most common valvular
lesion foundin pregnancy. The stenotic mitral valve causes
decreasedleft ventricle lling and can ultimately lead to pulmonary
hypertension and right ventricle failure. Individuals whohave
mitral stenosis warrant an echocardiogram and anelectrocardiogram.
Patients must be carefully monitoredfor pulmonary edema and can
experience atrial brillation
and arrhythmias. Anticoagulation should be considered,especially
if the patient experiences atrial brillation. Med-ications that
cause tachycardia (eg, terbutaline) should beavoided, and an
assisted second stage of labor to decreaseuse of Valsalva maneuvers
should be strongly considered.
Aortic StenosisPregnant patients who have aortic stenosis (AS)
generally tolerate pregnancy well if their disease is mild
(valvulararea > 1.5 cm 2 ). If the valve becomes more
stenotic
and is decreased to one fourth the normal 3 to 4 cm 2
in diameter, then the disease is considered severe, andsurgical
repair is recommended. The cardiac output forthese patients is xed,
due to the stenotic aortic valve,making proper perfusion of the
mother, as well as the fe-tus, dif cult. For this reason, patients
who have severe AS(aortic valve < 1 cm2 ) should limit their
physical activity.Patients should have an electrocardiogram to look
for ar-rhythmias and an echocardiogram to evaluate the aortic valve
and ejection fraction. It is imperative to maintainan appropriate
preload as these patients will not be ableto increase cardiac
output, which is needed to maintainperfusion during the physiologic
stresses of pregnancy.For the same reasons, hypotension and
bradycardia shouldbe avoided. Useof a narcotic epidural is
possible, but great care must be taken to avoid hypotension with
placement of any epidural catheter. Patient symptoms should be
moni-tored often to precisely decide on NYHA classi cation of the
pregnant patient who has AS, and placental perfusion will need to
be evaluated throughout the pregnancy.
Counseling patients who have a valvular lesion variesdepending
on the type of lesion and degree of effect.Low-risk lesions such as
issues with the tricuspid valve,pulmonary stenosis, mitral valve
prolapse, and regurgi-tant lesions of the mitral or aortic valve
are well toleratedin pregnancy and often do not require further
evaluation.
Stenotic lesions of the mitral or aortic valve can
causecomplications and must be more carefully managed dur-ing
pregnancy. Combining maternal NYHA classi cationas well as maternal
history with the valvular heart lesion(Table 4) can help in
counseling the pregnant patient re-garding maternal and fetal
risks.
Peripartum CardiomyopathyDiagnosis of peripartum cardiomyopathy
classically is thedevelopment of cardiac failure (ejection fraction
< 45%)
Table 5. Management of Valvular Lesions in PregnancyLesion
Medical Management
PS Avoid: hypotension, bradycardia, myocardial depressants,
excess blood lossMR Avoid: arrhythmia, bradycardia, increase in
SVR, myocardial depressantsAR Avoid: arrhythmia, bradycardia,
increase in SVR, myocardial depressantsMS Avoid: tachycardia, uid
overload, decrease in SVR, hypotension, increase in PVR
Treatment: diuretics, b -blockers, maintain HR < 100 beats
per minuteASa Avoid: hypotension, decrease in venous return,
bradycardia
Treatment: b -blockers, aggressive uids to prevent
hypotension
AR aortic regurgitation; AS aortic stenosis; HR heart rate; MR
mitral regurgitation; MS mitral stenosis; SVR systemic vascular
resistance;PS pulmonary stenosis; PVR peripheral vascular
resistance.a No epidural.
maternal-fetal medicine cardiovascular
NeoReviews Vol.13 No.11 November 2012 e655
at Health Internetwork on January 27,
2013http://neoreviews.aappublications.org/ Downloaded from
http://neoreviews.aappublications.org/http://neoreviews.aappublications.org/http://neoreviews.aappublications.org/http://neoreviews.aappublications.org/
-
8/14/2019 Enfermedad Cardiovascular Materna
7/12
from the last month of pregnancy up to 5 months postpartum
withno identi able cause for cardiac fail-ure. This condition can
lead to ma-ternal mortality, and maternal deathis most common in
the immediatepostpartum period. Management details regarding the
patient whohas peripartum cardiomyopathy canbe found in Fig 3.
Anticoagulant therapy is not prophylactically war-rantedunless the
patienthas a knowncardiac thrombus or coronary artery disease.
Medication Use in PregnancyMedications can be used with carein
the pregnant cardiac patient (Fig 4). Most cardiac medicationsused
in pregnancy are the same asthose in the nonpregnant patient.For
example, if a pregnant patient is experiencing supraventricular
tachy-cardia requiring cardioversion oradenosine, both agents are
safe inpregnancy and should be adminis-
tered if necessary. Speci c cardiacdrugs that should be avoided
inpregnancy are angiotensin-convertingenzyme inhibitors and
angiotensinreceptor blockers. Exposure to thesemedications in the
rst trimester canlead to congenital malformations,including cardiac
defects such asPDA, ASD, and VSD. In the latertrimesters, the fetus
can experienceimpaired renal function causing de-creased amniotic
uid (oligohy-
dramnios) and ultimately neonatalrenal failure. The low uid in
uterocan lead to fetal pulmonaryhypoplasiaas well as contracted
limbs and ab-normal bone formation. Furthermore,
theneonateexposedto an angiotensin-converting enzyme inhibitor or
angio-tensin receptor blocker in the second or third trimestercan
experience retinopathy or hypotension.
Anticoagulation in PregnancyUnfractionated heparin (UFH) and
low-molecular-weight heparin are considered safe in pregnancy and
do not cross the placenta. UFH has a shorter half-life than
low-molecular-weight heparin (Table 6) and thereforeis often the
preferred anticoagulant used when a preg-nancy nears term. Either
drug may be reversed with prot-amine sulfate, with the obvious fact
that reversal will befaster with UFH. In general,
low-molecular-weight hep-arin is preferred to UFH because there is
often lessfrequent dosing required, decreased risk for
heparin-induced thrombocytopenia, and a lower rate of osteopo-rosis
and skin reactions.
Figure 3. Management after diagnosis of peripartum
cardiomyopathy. ACE [ angiotensin-converting enzyme; CAD[ coronary
artery disease; CCB[ calcium channel blocker; IV [intravenous;
LMWH[ low-molecular-weight heparin; LV [ left ventricular; SBP[
systolicblood pressure; UFH[ unfractionated heparin.
maternal-fetal medicine cardiovascular
e656 NeoReviews Vol.13 No.11 November 2012
at Health Internetwork on January 27,
2013http://neoreviews.aappublications.org/ Downloaded from
http://neoreviews.aappublications.org/http://neoreviews.aappublications.org/http://neoreviews.aappublications.org/http://neoreviews.aappublications.org/
-
8/14/2019 Enfermedad Cardiovascular Materna
8/12
Warfarin, however, crosses the placenta and is usually not used
in pregnancy. Use in the rst trimester warrantsconcern for fetal
malformations such as nasal and limb
hypoplasia, optic atrophy, and impaired mental status.The risk
of this syndrome, referred to as warfarin
embryopathy, is estimated by Hirschand Fuster to be 4% to 10%.
More-over, use of warfarin during em-bryogenesis in the rst
trimester isrelated to higher miscarriage rates.During the latter
part of pregnancy,use of warfarin can have a deleteri-ous effect on
the fetus, sometimesresulting in intracranial hemor-rhage. It is
also important to notethe long half-life of warfarin, espe-cially
when compared with theother anticoagulant choices (Table6). In a
study byChan etal, warfarin was found to be more effective thanUFH
in preventing venous throm-boembolism in patients who
haveolder-generation mechanical heart valves. With the risks of
warfarin,and the availability of other anti-coagulant agents that
are highly effective in preventing venousthromboembolism, warfarin
isnot routinely used in the pregnant patient.
Systemic BacterialEndocarditis ProphylaxisPregnant patients who
have cardiaclesions do not require antibioticprophylaxis.
Currently, the Ameri-can College of Obstetricians andGynecologists,
as well as the Amer-ican Heart Association, recommendsystemic
bacterial endocarditis pre-
vention with a vaginal or cesarean delivery only if infec-tion
is present in speci c cardiac lesions (Table 7). Theantibiotics
recommended are as follows: ampicillin, cefa-
zolin, ceftriaxone, clindamycin, or amoxicillin.
Becausecefazolin, ceftriaxone, and clindamycin do not cover
en-terococcus, vancomycin should be added to those regi-mens.
Antibiotics should be administered 30 to 60minutes before
delivery.
ConclusionsCardiac lesions in pregnancy are often well
tolerated, but those that are not warrant a cardiac evaluation as
well ascareful management in the antepartum and peripartumperiods.
Many patients, speci cally those who have peri-partum
cardiomyopathy, are at a higher risk of death in
Figure 4. Fetal effects of cardiac medications in pregnancy.
Drug classes are given inparentheses. The classes are: (A), human
studies show no risk to fetus; (B), animal studiesshow risk or no
risk to fetus, but human studies show no risk to fetus; (C), animal
studieshave shown adverse risk to fetus, but human studies are
lacking; (D), human studies showevidence of fetal risk. Class C and
D may have medical benets for the mother that couldoutweigh risk to
fetus. IUGR[ intrauterine growth retardation.
Table 6. AnticoagulationMedications
Anticoagulant Half-Life
Unfractionated heparin 6090 minLow-molecular-weight heparin 4.5
h (single dose)
7 h (multiple doses)Warfarin 1.52.5 d
maternal-fetal medicine cardiovascular
NeoReviews Vol.13 No.11 November 2012 e657
at Health Internetwork on January 27,
2013http://neoreviews.aappublications.org/ Downloaded from
http://neoreviews.aappublications.org/http://neoreviews.aappublications.org/http://neoreviews.aappublications.org/http://neoreviews.aappublications.org/
-
8/14/2019 Enfermedad Cardiovascular Materna
9/12
the immediate postpartum period. One cannot forget that the
postpartum period is an important time to watchthe cardiac patient
closely because third-spacing andincreased cardiac output can put
added stress on an al-ready inadequately functioning heart. It is
important toproperly identify the exact cardiac lesions a pregnant
woman presents with and closely monitor her symptoms(with
assistance of NYHA classi cation) so that she canbe properly
counseled, managed, and treated throughout her pregnancy.
Suggested Reading American College of Obstetricians and
Gynecologists. Practice
bulletin no. 120: use of prophylactic antibiotics in labor
anddelivery. Obstet Gynecol . 2011;117:1472 1483
American College of Cardiology/American Heart Association Task
Force on Practice Guidelines; Society of Cardiovascular Anes-
thesiologists; Society for Cardiovascular Angiography and Inter-
ventions; Society of Thoracic Surgeons; Bonow RO, CarabelloBA, Kanu
C, et al. ACC/AHA 2006 guidelines for themanagement of patients
with valvular heart disease: a report of the American College of
Cardiology/American Heart AssociationTask Force on Practice
Guidelines (writing committee to revise the1998 Guidelines for the
Management of Patients With ValvularHeart Disease): developed in
collaboration with the Society of Cardiovascular Anesthesiologists:
endorsed by the Society forCardiovascular Angiography and
Interventions and the Society of Thoracic Surgeons. Circulation .
2006;114(5):e84 e231
Bonow RO, Carabello BA, Chatterjee K, et al. 2008 Focusedupdate
incorporated into the ACC/AHA 2006 Guidelines forthe Management of
Patients With Valvular Heart Disease:a report of the American
College of Cardiology/AmericanHeart Association Task Force on
Practice Guidelines (WritingCommittee to revise the 1998 guidelines
for the management of patients with valvular heart disease)
endorsed by the Society of Cardiovascular Anesthesiologists,
Society for Cardiovascular Angiography and Interventions, and
Society of ThoracicSurgeons. J Am Coll Cardiol . 2008;52(13):e1
e142
Chan WS, Anand S, Ginsberg JS. Anticoagulation of pregnant women
with mechanical heart valves: a systematic review of theliterature.
Arch Intern Med . 2000;160(2):191 196
Chang J, Elam-Evans LD, Berg CJ, et al.
Pregnancy-relatedmortality surveillance United States, 1991-1999.
MMWR Surveill Summ . 2003;52(2):1 8
Donnelly JE, Brown JM, Radford DJ. Pregnancy outcome andEbstein
s anomaly. Br Heart J . 1991;66(5):368 371
Francois K. Postpartum hemorrhage. In: Foley MR, Strong
TH,Garite TJ, eds. Obstetric Intensive Care Manual . 3rd ed.New
York, NY: The McGraw-Hill Companies Inc; 2010:27 37
Hirsch J, Fuster V. Guide to anticoagulant therapy. Part 2:
oralanticoagulants. American Heart Association. Circulation .
1994;89(3):1469 1488
Lupton M, Oteng-Ntim E, Ayida G, Steer PJ. Cardiac disease
inpregnancy. Curr Opin Obstet Gynecol . 2002;14(2):137 143
Martin SR, Hill AJ, Foley MR. Cardiac disease in pregnancy.
In:Queenan JT, Spong CY, Lockwood CJ. eds. Queenan s Management of
High-Risk Pregnancy . 6th ed. Oxford: Wiley-Blackwell; 2012:260
291
Simpson LL. Maternal cardiac disease: update for the
clinician.Obstet Gynecol . 2012;119(2 pt 1):345 359
Vandvik PO, Lincoff AM, Gore JM, et al; American College of
Chest Physicians. Primary and secondary prevention of cardio-
vascular disease: antithrombotic therapy and prevention of
thrombosis, 9th ed: American College of Chest
PhysiciansEvidence-Based Clinical Practice Guidelines [published
correc-tion appears in Chest . 2012;141(4):1129]. Chest .
2012;141(suppl 2):e637S e668S
Table 7. Cardiac Lesions RequiringSystemic Bacterial
EndocarditisProphylaxis When Infection IsPresent Prosthetic cardiac
valve or prosthetic material for valve
repair History of infective endocarditis Unrepaired cyanotic CHD
(palliative shunts, conduits) Completely repaired CHD with
prosthetic materials if
done < 6 mo ago Repaired CHD with residual defects
CHD
congenital heart disease.
American Board of Pediatrics Neonatal-PerinatalMedicine Content
Specications Know the effects on the fetus and/or
newborn infant of maternal cardiacdisease and its
management.
Know the effects on the fetus and/ornewborn infant of
maternalthromboembolic, or potentialthromboembolic (eg articial
valve), disorders and theirmanagement, including the use of
anticoagulant agents.
maternal-fetal medicine cardiovascular
e658 NeoReviews Vol.13 No.11 November 2012
at Health Internetwork on January 27,
2013http://neoreviews.aappublications.org/ Downloaded from
http://neoreviews.aappublications.org/http://neoreviews.aappublications.org/http://neoreviews.aappublications.org/http://neoreviews.aappublications.org/
-
8/14/2019 Enfermedad Cardiovascular Materna
10/12
NeoReviews QuizNew Minimum Performance Level RequirementsPer the
2010 revision of the American Medical Association (AMA) Physicians
Recognition Award (PRA) and creditsystem, a minimum performance
level must be established on enduring material and journal-based
CME activities thatare certied for AMA PRA Category 1 Credit TM .
In order to successfully complete 2012 NeoReviews articles for
AMAPRA Category 1 Credit TM , learners must demonstrate a minimum
performance level of 60% or higher on thisassessment, which
measures achievement of the educational purpose and/or objectives
of this activity.
Starting with 2012 NeoReviews , AMA PRA Category 1 Credit TM can
be claimed only if 60% or more of the questionsare answered
correctly. If you score less than 60% on the assessment, you will
be given additional opportunities toanswer questions until an
overall 60% or greater score is achieved.
1. A 25-year-old woman is in her second trimester of pregnancy.
She has been referred to the high risk obstetric
clinic for cardiac disease. Prior to more extensively reviewing
her history, doing a physical exam, and additionalevaluation, you
think about some of the most common congenital heart diseases seen
in the pregnant patientand consider their relative consequences
during pregnancy. Which of the following is correct about
possiblecongenital heart disease in this pregnant woman?A. Atrial
septal defect is one of the least common lesions encountered in the
pregnant patient.B. If coarctation of the aorta is present,
Valsalva maneuver during the second stage of labor should be
encouraged.C. Most patients with Tetralogy of Fallot who become
pregnant have had no previous operation on their
cardiac lesion.D. Patent ductus arteriosus is encountered often
and is tolerated poorly in pregnancy.E. The leading causes of
maternal mortality during pregnancy consist of cardiomyopathy,
pulmonary
hypertension, aortic dissection and myocardial infarction.
2. You consider some of the physiologic changes that occur
during pregnancy that may affect cardiovascularstatus and their
clinical implications for the mother and the fetus. Which of the
following is correct?A. Blood volume increases.B. Cardiac output
decreases.C. Heart rate decreases.D. Stroke volume decreases.E.
Systemic vascular resistance increases.
3. You notice that this mother is tall, and you consider the
possibility of Marfan syndrome. Which of thefollowing is correct
about a pregnant woman with Marfan syndrome?A. It would be very
unusual for her to have a baby who also has Marfan syndrome.B.
Marfan syndrome is autosomal recessive and seldom is accompanied by
cardiac complications.C. Pre-pregnancy aortic repair is not
indicated if the dilation of the aorta is more than 4.5 cm because
the risk
of rupture is low, especially if the mother is asked to do
strong Valsalva maneuvers during the second stage
of labor.D. Pre-pregnancy aortic repair is required even if the
aorta does not show dilation.E. The main concern is that dilation
of the aortic root could lead to dissection and aortic rupture.
4. After the physical exam, you are concerned that the woman has
a valvular abnormality of her heart. Which of the following is
correct?A. Mitral stenosis is the least common valvular lesion
found in pregnancy.B. Most of the valvular lesions seen in
pregnancy are acquired from rheumatic fever.C. Physical exertion
need not be limited in pregnant women with aortic stenosis when
their valves are stenotic
to more than 1/4 th of normal.D. Regurgitant lesions in the
mitral and aortic valves are much more worrisome than stenotic
lesions of these
valves.E. There is no need for anticoagulation in a woman who
has mitral stenosis and atrial brillation.
maternal-fetal medicine cardiovascular
NeoReviews Vol.13 No.11 November 2012 e659
at Health Internetwork on January 27,
2013http://neoreviews.aappublications.org/ Downloaded from
http://neoreviews.aappublications.org/http://neoreviews.aappublications.org/http://neoreviews.aappublications.org/http://neoreviews.aappublications.org/
-
8/14/2019 Enfermedad Cardiovascular Materna
11/12
5. In terms of cardiac medications used in pregnancy, which of
the following is correct?A. Adenosine should not be administered to
a pregnant patient who is experiencing supraventricular
tachycardia.B. Angiotensin converting enzyme inhibitors and
angiotensin receptor blockers should be avoided in the rst
trimester because they can lead to congenital malformations and
in the later trimesters the fetus canexperience impaired renal
function that can result in oligohydramnios.
C. Antibiotic prophylaxis should not be used in pregnant women
with cardiac lesions even if they haveinfective endocarditis.
D. Unfractionated heparin and low molecular weight heparin are
safe for the fetus because they readily crossthe placenta.
E. Warfarin is a safe drug to use for anticoagulation during all
stages of pregnancy.
maternal-fetal medicine cardiovascular
e660 NeoReviews Vol.13 No.11 November 2012
at Health Internetwork on January 27,
2013http://neoreviews.aappublications.org/ Downloaded from
http://neoreviews.aappublications.org/http://neoreviews.aappublications.org/http://neoreviews.aappublications.org/http://neoreviews.aappublications.org/
-
8/14/2019 Enfermedad Cardiovascular Materna
12/12
DOI: 10.1542/neo.13-11-e6512012;13;e651 Neoreviews
Alexandria J. Hill and Luis D. PachecoCardiovascular Disease in
Pregnancy
ServicesUpdated Information &
http://neoreviews.aappublications.org/content/13/11/e651including
high resolution figures, can be found at:
References
http://neoreviews.aappublications.org/content/13/11/e651#BIBL
This article cites 8 articles, 2 of which you can access for
free at:
Subspecialty Collections
orn_infanthttp://neoreviews.aappublications.org/cgi/collection/fetus_newbFetus
and Newborn Infantlar_disorders
http://neoreviews.aappublications.org/cgi/collection/cardiovascuCardiovascular
Disordersfollowing collection(s):This article, along with others on
similar topics, appears in the
Permissions & Licensing
/site/misc/Permissions.xhtmltables) or in its entirety can be
found online at:Information about reproducing this article in parts
(figures,
Reprints /site/misc/reprints.xhtmlInformation about ordering
reprints can be found online: