Embed Size (px)
Citation preview

Kroacutenikus faacutejdalom idegsebeacuteszeti kezeleacutese
Balaacutes Istvaacuten
PTE AacuteOK Idegsebeacuteszeti Klinika
Kroacutenikus faacutejdalom tiacutepusai
bull Nociceptiacutev
bull Nem nociceptiacutev
Nociceptiacutev faacutejdalom
bull Faacutejdalmas ( nociceptiv) ingerrel kivaacuteltott a perifeacuteriaacutes nociceptorok kroacutenikus aktivaacutecioacuteja vagy tuacutelaktivaacuteloacutedaacutesa (pl degeneratiacutev esetleg daganatos eredetű laacutegyreacutesz izuumlleti vagy csontfolyamatok)
bull eacuteles markoloacute
bull csillapiacutethatoacute oacutepiaacutetokkal
bull nincs idegrendszeri tuumlnet (eacuterzeacuteszavar) a faacutejdalmas teruumlleten
Neuropathiaacutes neurogeacuten faacutejdalom
bull Idegrendszeri seacuteruumlleacutes (eacuterzőpaacutelya) koumlvetkezmeacutenye
bull Idegrendszeri tuumlnet
bull Faacutejdalomvezető paacutelyaacutek innervaacutecioacutejaacutenakelveszteacutese
bull Eacutegő eacuterzeacuteszavar
bull Nem reagaacutel opiaacutetokra
Neuropathiaacutes neurogeacuten faacutejdalomjellemzői
bull Thermaacutelis (eacutegő hideg)
bull exteroceptiv (elektromos villaacutemlaacutesszerűcsiacutepő szuacuteroacute)
dysaesthesia
bull Proprioceptiv (szaggatoacute szoriacutetoacute markoloacute)
aacutellandoacute időszakos kuumllső ingerekkel kivaacutelthatoacute (thermaacutelis tactilis proprioceptiv allodynia hyperalgeacutezia)
Idegsebeacuteszeti faacutejdalomcsillapiacutetaacutesi lehetőseacutegek neuropaacutetiaacutes faacutejdalomban
bull Ablatiacutev
bull Neuromodulaacutecioacute
Ablatiacutev faacutejdalomcsillapiacutetoacute idegsebeacuteszeti beavatkozaacutesok
bull faacutejdalomvezető paacutelyaacutekat aacutetmetszeacutese roncsolaacutesa destruktiacutev (rizotomiaDREZmyelotomiatermocoagulaacutecioacute)
bull szaacutemos esetben hataacutestalan bull hataacutes aacutetmenetibull maradandoacute hiaacutenytuumlnetbull irreverzibilis magasabb morbiditaacutes bull deafferentaacutecioacutes faacutejdalmak kialakulaacutesa
Funkcionaacutelis idegsebeacuteszetdefiniacutecioacute
bull Koacuteros idegrendszeri műkoumldeacutesek (funkcioacutek) műteacuteti uacuteton toumlrteacutenő befolyaacutesolaacutesa (normalizaacutelaacutesa)
Funkcionaacutelis idegsebeacuteszet -alkalmazaacutesi teruumlletek
bull kroacutenikus faacutejdalom
bull mozgaacuteszavarok
bull spasticitaacutes
bull epilepszia
bull psychochirurgia
bull vegetatiacutev zavarok
Neuromodulaacutecioacute
bull centraacutelis-perifeacuteriaacutes-autonom idegrendszer műkoumldeacuteseacutenek teraacutepiaacutes alteraacutecioacuteja
bull implantaacutelt keacuteszuumlleacutek
bull elektromos gyoacutegyszeres
bull non-destruktiacutev
bull reverzibilis
bull betegseacuteget nem gyoacutegyiacutet
bull műkoumldeacutest eacuteletminőseacuteget javiacutet
Neuromodulaacutecioacute tiacutepusai
bull Elektromos (neurostimulaacutecioacute)
bull Keacutemiai (gyoacutegyszerpumpa)
Neuropathic pain
bull International Association for the Study of Pain defines pain caused by a lesion or disease of the somatosensory nervous system
bull suffer more often from insomnia anxiety and depression1
bull analgetic medication insufficient2
bull SCS has undergone constant technical advancement
Why Neuromodulation
bull Testable
bull Completely reversible
bull Non-destructive
bull No limitation to future therapy
Neurostimulaacutecioacute helye
bull perifeacuteriaacutes ideg PNS PNfS DRGS
bull gerincvelő SCS
bull meacutelyagyi DBS
bull motoros agykeacutereg MCS
Neurostimulaacutecioacutes faacutejdalomcsillapiacutetoacute műteacutetek indikaacutecioacutejaacutenak felaacutelliacutetaacutesa
bull faacutejdalom kezeleacuteseacuteben jaacuteratos szakemberek koumlzoumls doumlnteacutese
bull centrumokban (kivizsgaacutelaacutes kezeleacutes szoumlvődmeacutenyek elhaacuteriacutetaacutesa)
bull multidisciplinaacuteris (ideggyoacutegyaacutesz idegsebeacutesz psychiaacuteter psycholoacutegus anaesthesioloacutegus neuroradioloacutegus elektrofizioloacutegus mozgaacutesterapeuta) munkacsoport
Neurostimulaacutecioacute aacuteltalaacutenos kontraindikaacutecioacutek
(kroacutenikus faacutejdalom)
bull psychiaacutetriai koacuterkeacutepek (aktiacutev psychosis suacutelyos depresszioacute hipochondria szomatizaacutecioacutes betegseacutegek)
bull nem egyuumlttműkoumldő beteg
bull alkoholizmus kaacutebiacutetoacuteszer-eacutelvezet
bull suacutelyos kiacuteseacuterő betegseacuteg (coagulopathia immundeficiencia)
bull maacutes implantaacutelt pacemaker (pl sziacutev)
Neurostimulaacutecioacute műteacuteti szoumlvődmeacutenyek
bull korrigaacutelhatoacutek
bull implantaacutetummal (8-10) kapcsolatos
(elektroacuteda elmozdulaacutes seacuteruumlleacutes elektromos műkoumldeacutes zavar)
bull veacuterzeacutesek (1-5)
bull gyulladaacutesok (5-7)
Spinal cord stimulaacutecioacute (SCS)
bull Legneacutepszerűbb leggyakrabban alkalmazott
bull Első SCS daganatos faacutejdalom (Shealey 1967)
History of Spinal Cord StimulationShealy 1969
bull 1967 ndash Long and Wall PNS
bull 1969 ndash Shealy SCS in humans
bull 1975 ndash Dooley perc electrode
bull Mid 1970s ndash self-powered battery
bull 1980s - programmable quad electrode
bull 1980s -1990s ndash Primary cell IPG
bull 2004 ndash Rechargeable IPG
Clinical studies on SCS continue to support the effectiveness of this
therapy The following charts summarize studies of SCS and its
effects on the quality of life of patients
Reduction of Pain
ReferenceNumber of
PatientsFollow Up Results
Kumar17 410 8 years 74 had gt50 relief
North14 19 3 years 47 had gt50 relief
Barolat9 41 1 year50-65 had good to
excellent relief
Van Buyten18 123 3 years68 had good to excellent
relief
Cameron19 747Up to 59 months
(49 years)
62 had gt50 relief or
significantly reduced pain
scores
SCS indikaacutecioacutek INeuropaacutethiaacutes (neurogeacuten) faacutejdalom
bull Perifeacuteriaacutes idegek seacuteruumlleacutese gyoumlkoumlk plexusok (idegrendszeri hiaacutenytuumlnet) seacuteruumlleacutes okai baleseti műteacutet pl lumbaacutelis discectomia (gyoumlk) nőgyoacutegyaacuteszati (inguinalis ideg) teacuterdműteacutetek (infrapatellaacuteris ideg) mastectomia (costo-brachiaacutelis ideg)
bull veacutegtag-amputaacutecioacute csonkfaacutejdalom jobban mint a fantom faacutejdalombull post-herpeses neuralgia amennyiben a bőreacuterzeacutes reacuteszlegesen megtartottbull post-irradiaacutecioacutes plexopaacutetiabull polyneuropaacutetiaacutek (diabeteses alkoholos) post-kemoteraacutepiaacutes (amennyiben a vastag rostok
műkoumldeacutese reacuteszlegesen megtartott)bull gerincvelő incomplett seacuteruumlleacutese -amennyiben a vastag eacuterzőrostok műkoumldeacutese megtartott eacutes a
segmentaacutelis faacutejdalom a seacuteruumlleacutes magassaacutegaacuteban leacutep felbull cervicaacutelis eacutes lumbosacralis radiculopaacutetiaacutek (compresszioacute ischaemia sebeacuteszi baleset
arachnoiditisbull CRPS II (causalga)bull DE bull plexus avulsioacute syringomyelia faacutejdalom nem csillapiacutethatoacutek bull nincs egyeteacuterteacutes a CRPS I (reflex sympaticus dystrophia)
SCS indikaacutecioacutek II
bull Kevert faacutejdalom szindroacutemaacutek
Falied back surgery syndroma = FBSS koraacutebbi gerincsebeacuteszeti beavatkozaacutes (postoperatiacutev fibrosis arachnoiditis)
Posztlaminektomiaacutes szindroacutemaangolszaacutesz failed back surgery szindroacutemaacutenak (FBSS)
bull faacutejdalom lokalizaacutecioacute alsoacute aacutegyeacuteki gerinc far
alsoacute veacutegtagok
bull etioloacutegia arachnoiditis epiduraacutelis heg
radiculitis mikro-instabilitaacutes rec
porckorongseacuterv gyulladaacutes
bull tapasztalatok alsoacute veacutegtagba terjedő
faacutejdalomra SCS hateacutekony
bull axiaacutelis faacutejdalmakra nem bizonyiacutetott
Incidencia FBSS
bull ranges 5 - 50
bull postdiscectomy 10-40
Etiologia FBSS
bull Scar tissue that forms around the surgery site interrupting normal neurological functioning
bull technicalities of the operation are not successful the performing surgeon had poor technique andor there is iatrogenic injury present
bull surgery is not performed at the site that causes the pain
bull surgery performed is not actually necessarybull patient is a poor fit for a successful surgerybull diagnosis was incorrectbull Complications of surgery arise
1 Anderson VC et al Current review of pain 20004105-11 5 Vaccaro AR et al Spine 200126 (24) S111-82 Leveque JC et al Neuromodulation 200141-9 6 Spengler DM et al Spine 19805356-603 Dario A et al Neuromodulation 20014105-110 7 Fager CA Freidberg SR Spine 1980587-944 Ohnmeiss DD et al The Spine Journal 2001358-363 8 Long DM Surgical management of pain 2002 354-64
FBSS okai eacutes tuumlnetei
bull FBSS cause1-7
ndash irreversible nerve injury
ndash surgical complications
ndash psychosocial problems
ndash inappropriate selection of patients for surgery
ndash recurrent herniation
ndash wrong level of operation
bull FBSS symptoms348
ndash lumbosacral postoperative fibrosis andor arachnoiditis
ndash root lesion
ndash dorsal compartment syndrome
ndash lateral spinal stenosis
SCS indikaacutecioacutek IIIAngina pectoris
bull New York Heart Association III-IV csoport (szignifikaacutens coronaacuteria stenosis egy vagy toumlbb szűkuumllet 70 )
bull myocardiaacutelis ischaemia reverzibilis angina gyoacutegyszeres revascularizaacutecioacutes beavatkozaacutesokkal nem enyhiacutethető
bull eacuteletminőseacuteguarr nitro-glicerin felhasznaacutelaacutesdarr anginaacutes rohamok szaacutemadarr jaacuteraacutestaacutevolsaacuteguarr
bull SCS anti-ischaemiaacutes hataacutes
bull nincs bizonyiacuteteacutek SCS hateacutekonysaacutegra instabil angina acut myocardiaacutelis infarctus vazospasticus angia maacutes sziacutevbetegseacuteg okozta anginaacutes faacutejdalmak csillapiacutetaacutesaacutera
Anginaacutes faacutejdalom
SCS tanulmaacutenyok hateacutekonysaacuteg I
bull Nienke (45 ) PT 1 eacutev koumlveteacutes eacuteletminőseacuteg szociaacutelis mentaacutelis fizikaacutelis teljesiacutetmeacuteny szignifikaacutensan javul
bull Hautvast (46) stabil angina pectorisban RT 6 heacutet koumlveteacutes
Randomizaacutelaacutes a stimulaacutetor OFF b csoport 3x1 oacuteranap ON vagy hirtelen anginaacuteban
anginaacutes rohamszaacutem csoumlkken
fizikai teljesiacutetőkeacutepesseacuteg javul
sublinguaacutelis nitraacutet felhasznaacutelaacutes csoumlkken
EKG-n az ischaemiaacutes epizoacutedusok csoumlkkennek
ST depresszioacute enyhuumll eacuteletminőseacuteg javul
anginaacutes faacutejdalom csoumlkken
SCS indikaacutecioacutek IIIAngina pectoris
bull tanulmaacutenyok eredmeacutenyei kedvezőek (39-43)
bull teraacutepiaacutes hataacutes hosszuacute taacutevuacute
bull nitraacutet bevitel csoumlkkenthető
bull faacutejdalomcsillapiacutetoacute hataacutesuacute
bull sziacutevizom veacuterkeringeacutes javul
bull PET tanulmaacuteny
ischaemiaacutes sziacutevizomban keringeacuteseacuteben
redistribucio alakul ki nyugalomban
eacutes gyoacutegyszer indukaacutelt stresszben(44)
SCS indikaacutecioacutek IVPerifeacuteriaacutes vasculaacuteris betegseacutegek
bull lassan progrediaacuteloacute perifeacuteriaacutes vasculaacuteris ischaemia -atherosclerosis (Fontaine 3 4 staacutedium )
bull vazospasticus betegseacuteg (pl Raynaud frostbite) gyoacutegyszeresen eacutersebeacuteszeti műteacutettel nem uralhatoacute veacutegtagfaacutejdalom
bull Buerger-koacuter
bull kontraindikaacutelt laacutebszaacuterfekeacutelygt 3 cm gangreacutena
SCS indikaacutecioacutek VCRPS
CRPS tuumlnetei
1 Harden RN et al Pain 199983211-219 6Birklein F et al Pain 19976949-54
2 Galer BS et al J Pain Symptom Manage 200020286-92 7 Schwartzman RJ Kerrigan J
Neurosurgery 19904057-61
3 Birklein F Handwerker HO Pain 2001 941-6 8 Zyluk A J Hand Surg 200126151-154
4 Rommel O et al Pain 19998095-101 9 Wasner G et al Neuro Clin
199816851-68
5 Thimineur M et al Clin J Pain 199814256-67
Sensory Motor dysfunctionIntense pain12 Weakness
Allodynia13 Decreased range of motion3
Hyperesthesia13 Tremor16
Hyperalgesia13 Dystonia7
Sensory deficits4 Myoclonus7
Decreased muscular strength8
Autonomic Dystrophic Swelling1 Increaseddecreased nailhair growth
Colourtemperature changes6 Skin changes (eg palor plantar fibrosis
Sweating abnormalities6 hyperkeratosis and thin glossy
skin9 )
Courtesy of Robert J Schwartzman MD
SCS indikaacutecioacutek VIAbdominaacutelis eacutes visceraacutelis faacutejdalom
szindroacutemaacutek
bull Faacutejdalom etioloacutegiaacuteja vaacuteltozatos
bull Ok gastrointestinaacutelis gastro-urinaacutelis
musculosceletaacutelis idegrendszeri
bull Megfigyeleacutes Th X myelotomia
daganatos pelvicus faacutejdalmat csillapiacutet
Mechanisms of SCS
bull Gate control theory
bull Direct inhibition of spinothalamic neurons
bull Descending modulatory effects
bull Alteration of sympathetic activity
bull Neurochemical modulation
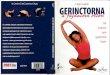
GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Kroacutenikus faacutejdalom tiacutepusai
bull Nociceptiacutev
bull Nem nociceptiacutev
Nociceptiacutev faacutejdalom
bull Faacutejdalmas ( nociceptiv) ingerrel kivaacuteltott a perifeacuteriaacutes nociceptorok kroacutenikus aktivaacutecioacuteja vagy tuacutelaktivaacuteloacutedaacutesa (pl degeneratiacutev esetleg daganatos eredetű laacutegyreacutesz izuumlleti vagy csontfolyamatok)
bull eacuteles markoloacute
bull csillapiacutethatoacute oacutepiaacutetokkal
bull nincs idegrendszeri tuumlnet (eacuterzeacuteszavar) a faacutejdalmas teruumlleten
Neuropathiaacutes neurogeacuten faacutejdalom
bull Idegrendszeri seacuteruumlleacutes (eacuterzőpaacutelya) koumlvetkezmeacutenye
bull Idegrendszeri tuumlnet
bull Faacutejdalomvezető paacutelyaacutek innervaacutecioacutejaacutenakelveszteacutese
bull Eacutegő eacuterzeacuteszavar
bull Nem reagaacutel opiaacutetokra
Neuropathiaacutes neurogeacuten faacutejdalomjellemzői
bull Thermaacutelis (eacutegő hideg)
bull exteroceptiv (elektromos villaacutemlaacutesszerűcsiacutepő szuacuteroacute)
dysaesthesia
bull Proprioceptiv (szaggatoacute szoriacutetoacute markoloacute)
aacutellandoacute időszakos kuumllső ingerekkel kivaacutelthatoacute (thermaacutelis tactilis proprioceptiv allodynia hyperalgeacutezia)
Idegsebeacuteszeti faacutejdalomcsillapiacutetaacutesi lehetőseacutegek neuropaacutetiaacutes faacutejdalomban
bull Ablatiacutev
bull Neuromodulaacutecioacute
Ablatiacutev faacutejdalomcsillapiacutetoacute idegsebeacuteszeti beavatkozaacutesok
bull faacutejdalomvezető paacutelyaacutekat aacutetmetszeacutese roncsolaacutesa destruktiacutev (rizotomiaDREZmyelotomiatermocoagulaacutecioacute)
bull szaacutemos esetben hataacutestalan bull hataacutes aacutetmenetibull maradandoacute hiaacutenytuumlnetbull irreverzibilis magasabb morbiditaacutes bull deafferentaacutecioacutes faacutejdalmak kialakulaacutesa
Funkcionaacutelis idegsebeacuteszetdefiniacutecioacute
bull Koacuteros idegrendszeri műkoumldeacutesek (funkcioacutek) műteacuteti uacuteton toumlrteacutenő befolyaacutesolaacutesa (normalizaacutelaacutesa)
Funkcionaacutelis idegsebeacuteszet -alkalmazaacutesi teruumlletek
bull kroacutenikus faacutejdalom
bull mozgaacuteszavarok
bull spasticitaacutes
bull epilepszia
bull psychochirurgia
bull vegetatiacutev zavarok
Neuromodulaacutecioacute
bull centraacutelis-perifeacuteriaacutes-autonom idegrendszer műkoumldeacuteseacutenek teraacutepiaacutes alteraacutecioacuteja
bull implantaacutelt keacuteszuumlleacutek
bull elektromos gyoacutegyszeres
bull non-destruktiacutev
bull reverzibilis
bull betegseacuteget nem gyoacutegyiacutet
bull műkoumldeacutest eacuteletminőseacuteget javiacutet
Neuromodulaacutecioacute tiacutepusai
bull Elektromos (neurostimulaacutecioacute)
bull Keacutemiai (gyoacutegyszerpumpa)
Neuropathic pain
bull International Association for the Study of Pain defines pain caused by a lesion or disease of the somatosensory nervous system
bull suffer more often from insomnia anxiety and depression1
bull analgetic medication insufficient2
bull SCS has undergone constant technical advancement
Why Neuromodulation
bull Testable
bull Completely reversible
bull Non-destructive
bull No limitation to future therapy
Neurostimulaacutecioacute helye
bull perifeacuteriaacutes ideg PNS PNfS DRGS
bull gerincvelő SCS
bull meacutelyagyi DBS
bull motoros agykeacutereg MCS
Neurostimulaacutecioacutes faacutejdalomcsillapiacutetoacute műteacutetek indikaacutecioacutejaacutenak felaacutelliacutetaacutesa
bull faacutejdalom kezeleacuteseacuteben jaacuteratos szakemberek koumlzoumls doumlnteacutese
bull centrumokban (kivizsgaacutelaacutes kezeleacutes szoumlvődmeacutenyek elhaacuteriacutetaacutesa)
bull multidisciplinaacuteris (ideggyoacutegyaacutesz idegsebeacutesz psychiaacuteter psycholoacutegus anaesthesioloacutegus neuroradioloacutegus elektrofizioloacutegus mozgaacutesterapeuta) munkacsoport
Neurostimulaacutecioacute aacuteltalaacutenos kontraindikaacutecioacutek
(kroacutenikus faacutejdalom)
bull psychiaacutetriai koacuterkeacutepek (aktiacutev psychosis suacutelyos depresszioacute hipochondria szomatizaacutecioacutes betegseacutegek)
bull nem egyuumlttműkoumldő beteg
bull alkoholizmus kaacutebiacutetoacuteszer-eacutelvezet
bull suacutelyos kiacuteseacuterő betegseacuteg (coagulopathia immundeficiencia)
bull maacutes implantaacutelt pacemaker (pl sziacutev)
Neurostimulaacutecioacute műteacuteti szoumlvődmeacutenyek
bull korrigaacutelhatoacutek
bull implantaacutetummal (8-10) kapcsolatos
(elektroacuteda elmozdulaacutes seacuteruumlleacutes elektromos műkoumldeacutes zavar)
bull veacuterzeacutesek (1-5)
bull gyulladaacutesok (5-7)
Spinal cord stimulaacutecioacute (SCS)
bull Legneacutepszerűbb leggyakrabban alkalmazott
bull Első SCS daganatos faacutejdalom (Shealey 1967)
History of Spinal Cord StimulationShealy 1969
bull 1967 ndash Long and Wall PNS
bull 1969 ndash Shealy SCS in humans
bull 1975 ndash Dooley perc electrode
bull Mid 1970s ndash self-powered battery
bull 1980s - programmable quad electrode
bull 1980s -1990s ndash Primary cell IPG
bull 2004 ndash Rechargeable IPG
Clinical studies on SCS continue to support the effectiveness of this
therapy The following charts summarize studies of SCS and its
effects on the quality of life of patients
Reduction of Pain
ReferenceNumber of
PatientsFollow Up Results
Kumar17 410 8 years 74 had gt50 relief
North14 19 3 years 47 had gt50 relief
Barolat9 41 1 year50-65 had good to
excellent relief
Van Buyten18 123 3 years68 had good to excellent
relief
Cameron19 747Up to 59 months
(49 years)
62 had gt50 relief or
significantly reduced pain
scores
SCS indikaacutecioacutek INeuropaacutethiaacutes (neurogeacuten) faacutejdalom
bull Perifeacuteriaacutes idegek seacuteruumlleacutese gyoumlkoumlk plexusok (idegrendszeri hiaacutenytuumlnet) seacuteruumlleacutes okai baleseti műteacutet pl lumbaacutelis discectomia (gyoumlk) nőgyoacutegyaacuteszati (inguinalis ideg) teacuterdműteacutetek (infrapatellaacuteris ideg) mastectomia (costo-brachiaacutelis ideg)
bull veacutegtag-amputaacutecioacute csonkfaacutejdalom jobban mint a fantom faacutejdalombull post-herpeses neuralgia amennyiben a bőreacuterzeacutes reacuteszlegesen megtartottbull post-irradiaacutecioacutes plexopaacutetiabull polyneuropaacutetiaacutek (diabeteses alkoholos) post-kemoteraacutepiaacutes (amennyiben a vastag rostok
műkoumldeacutese reacuteszlegesen megtartott)bull gerincvelő incomplett seacuteruumlleacutese -amennyiben a vastag eacuterzőrostok műkoumldeacutese megtartott eacutes a
segmentaacutelis faacutejdalom a seacuteruumlleacutes magassaacutegaacuteban leacutep felbull cervicaacutelis eacutes lumbosacralis radiculopaacutetiaacutek (compresszioacute ischaemia sebeacuteszi baleset
arachnoiditisbull CRPS II (causalga)bull DE bull plexus avulsioacute syringomyelia faacutejdalom nem csillapiacutethatoacutek bull nincs egyeteacuterteacutes a CRPS I (reflex sympaticus dystrophia)
SCS indikaacutecioacutek II
bull Kevert faacutejdalom szindroacutemaacutek
Falied back surgery syndroma = FBSS koraacutebbi gerincsebeacuteszeti beavatkozaacutes (postoperatiacutev fibrosis arachnoiditis)
Posztlaminektomiaacutes szindroacutemaangolszaacutesz failed back surgery szindroacutemaacutenak (FBSS)
bull faacutejdalom lokalizaacutecioacute alsoacute aacutegyeacuteki gerinc far
alsoacute veacutegtagok
bull etioloacutegia arachnoiditis epiduraacutelis heg
radiculitis mikro-instabilitaacutes rec
porckorongseacuterv gyulladaacutes
bull tapasztalatok alsoacute veacutegtagba terjedő
faacutejdalomra SCS hateacutekony
bull axiaacutelis faacutejdalmakra nem bizonyiacutetott
Incidencia FBSS
bull ranges 5 - 50
bull postdiscectomy 10-40
Etiologia FBSS
bull Scar tissue that forms around the surgery site interrupting normal neurological functioning
bull technicalities of the operation are not successful the performing surgeon had poor technique andor there is iatrogenic injury present
bull surgery is not performed at the site that causes the pain
bull surgery performed is not actually necessarybull patient is a poor fit for a successful surgerybull diagnosis was incorrectbull Complications of surgery arise
1 Anderson VC et al Current review of pain 20004105-11 5 Vaccaro AR et al Spine 200126 (24) S111-82 Leveque JC et al Neuromodulation 200141-9 6 Spengler DM et al Spine 19805356-603 Dario A et al Neuromodulation 20014105-110 7 Fager CA Freidberg SR Spine 1980587-944 Ohnmeiss DD et al The Spine Journal 2001358-363 8 Long DM Surgical management of pain 2002 354-64
FBSS okai eacutes tuumlnetei
bull FBSS cause1-7
ndash irreversible nerve injury
ndash surgical complications
ndash psychosocial problems
ndash inappropriate selection of patients for surgery
ndash recurrent herniation
ndash wrong level of operation
bull FBSS symptoms348
ndash lumbosacral postoperative fibrosis andor arachnoiditis
ndash root lesion
ndash dorsal compartment syndrome
ndash lateral spinal stenosis
SCS indikaacutecioacutek IIIAngina pectoris
bull New York Heart Association III-IV csoport (szignifikaacutens coronaacuteria stenosis egy vagy toumlbb szűkuumllet 70 )
bull myocardiaacutelis ischaemia reverzibilis angina gyoacutegyszeres revascularizaacutecioacutes beavatkozaacutesokkal nem enyhiacutethető
bull eacuteletminőseacuteguarr nitro-glicerin felhasznaacutelaacutesdarr anginaacutes rohamok szaacutemadarr jaacuteraacutestaacutevolsaacuteguarr
bull SCS anti-ischaemiaacutes hataacutes
bull nincs bizonyiacuteteacutek SCS hateacutekonysaacutegra instabil angina acut myocardiaacutelis infarctus vazospasticus angia maacutes sziacutevbetegseacuteg okozta anginaacutes faacutejdalmak csillapiacutetaacutesaacutera
Anginaacutes faacutejdalom
SCS tanulmaacutenyok hateacutekonysaacuteg I
bull Nienke (45 ) PT 1 eacutev koumlveteacutes eacuteletminőseacuteg szociaacutelis mentaacutelis fizikaacutelis teljesiacutetmeacuteny szignifikaacutensan javul
bull Hautvast (46) stabil angina pectorisban RT 6 heacutet koumlveteacutes
Randomizaacutelaacutes a stimulaacutetor OFF b csoport 3x1 oacuteranap ON vagy hirtelen anginaacuteban
anginaacutes rohamszaacutem csoumlkken
fizikai teljesiacutetőkeacutepesseacuteg javul
sublinguaacutelis nitraacutet felhasznaacutelaacutes csoumlkken
EKG-n az ischaemiaacutes epizoacutedusok csoumlkkennek
ST depresszioacute enyhuumll eacuteletminőseacuteg javul
anginaacutes faacutejdalom csoumlkken
SCS indikaacutecioacutek IIIAngina pectoris
bull tanulmaacutenyok eredmeacutenyei kedvezőek (39-43)
bull teraacutepiaacutes hataacutes hosszuacute taacutevuacute
bull nitraacutet bevitel csoumlkkenthető
bull faacutejdalomcsillapiacutetoacute hataacutesuacute
bull sziacutevizom veacuterkeringeacutes javul
bull PET tanulmaacuteny
ischaemiaacutes sziacutevizomban keringeacuteseacuteben
redistribucio alakul ki nyugalomban
eacutes gyoacutegyszer indukaacutelt stresszben(44)
SCS indikaacutecioacutek IVPerifeacuteriaacutes vasculaacuteris betegseacutegek
bull lassan progrediaacuteloacute perifeacuteriaacutes vasculaacuteris ischaemia -atherosclerosis (Fontaine 3 4 staacutedium )
bull vazospasticus betegseacuteg (pl Raynaud frostbite) gyoacutegyszeresen eacutersebeacuteszeti műteacutettel nem uralhatoacute veacutegtagfaacutejdalom
bull Buerger-koacuter
bull kontraindikaacutelt laacutebszaacuterfekeacutelygt 3 cm gangreacutena
SCS indikaacutecioacutek VCRPS
CRPS tuumlnetei
1 Harden RN et al Pain 199983211-219 6Birklein F et al Pain 19976949-54
2 Galer BS et al J Pain Symptom Manage 200020286-92 7 Schwartzman RJ Kerrigan J
Neurosurgery 19904057-61
3 Birklein F Handwerker HO Pain 2001 941-6 8 Zyluk A J Hand Surg 200126151-154
4 Rommel O et al Pain 19998095-101 9 Wasner G et al Neuro Clin
199816851-68
5 Thimineur M et al Clin J Pain 199814256-67
Sensory Motor dysfunctionIntense pain12 Weakness
Allodynia13 Decreased range of motion3
Hyperesthesia13 Tremor16
Hyperalgesia13 Dystonia7
Sensory deficits4 Myoclonus7
Decreased muscular strength8
Autonomic Dystrophic Swelling1 Increaseddecreased nailhair growth
Colourtemperature changes6 Skin changes (eg palor plantar fibrosis
Sweating abnormalities6 hyperkeratosis and thin glossy
skin9 )
Courtesy of Robert J Schwartzman MD
SCS indikaacutecioacutek VIAbdominaacutelis eacutes visceraacutelis faacutejdalom
szindroacutemaacutek
bull Faacutejdalom etioloacutegiaacuteja vaacuteltozatos
bull Ok gastrointestinaacutelis gastro-urinaacutelis
musculosceletaacutelis idegrendszeri
bull Megfigyeleacutes Th X myelotomia
daganatos pelvicus faacutejdalmat csillapiacutet
Mechanisms of SCS
bull Gate control theory
bull Direct inhibition of spinothalamic neurons
bull Descending modulatory effects
bull Alteration of sympathetic activity
bull Neurochemical modulation
GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Nociceptiacutev faacutejdalom
bull Faacutejdalmas ( nociceptiv) ingerrel kivaacuteltott a perifeacuteriaacutes nociceptorok kroacutenikus aktivaacutecioacuteja vagy tuacutelaktivaacuteloacutedaacutesa (pl degeneratiacutev esetleg daganatos eredetű laacutegyreacutesz izuumlleti vagy csontfolyamatok)
bull eacuteles markoloacute
bull csillapiacutethatoacute oacutepiaacutetokkal
bull nincs idegrendszeri tuumlnet (eacuterzeacuteszavar) a faacutejdalmas teruumlleten
Neuropathiaacutes neurogeacuten faacutejdalom
bull Idegrendszeri seacuteruumlleacutes (eacuterzőpaacutelya) koumlvetkezmeacutenye
bull Idegrendszeri tuumlnet
bull Faacutejdalomvezető paacutelyaacutek innervaacutecioacutejaacutenakelveszteacutese
bull Eacutegő eacuterzeacuteszavar
bull Nem reagaacutel opiaacutetokra
Neuropathiaacutes neurogeacuten faacutejdalomjellemzői
bull Thermaacutelis (eacutegő hideg)
bull exteroceptiv (elektromos villaacutemlaacutesszerűcsiacutepő szuacuteroacute)
dysaesthesia
bull Proprioceptiv (szaggatoacute szoriacutetoacute markoloacute)
aacutellandoacute időszakos kuumllső ingerekkel kivaacutelthatoacute (thermaacutelis tactilis proprioceptiv allodynia hyperalgeacutezia)
Idegsebeacuteszeti faacutejdalomcsillapiacutetaacutesi lehetőseacutegek neuropaacutetiaacutes faacutejdalomban
bull Ablatiacutev
bull Neuromodulaacutecioacute
Ablatiacutev faacutejdalomcsillapiacutetoacute idegsebeacuteszeti beavatkozaacutesok
bull faacutejdalomvezető paacutelyaacutekat aacutetmetszeacutese roncsolaacutesa destruktiacutev (rizotomiaDREZmyelotomiatermocoagulaacutecioacute)
bull szaacutemos esetben hataacutestalan bull hataacutes aacutetmenetibull maradandoacute hiaacutenytuumlnetbull irreverzibilis magasabb morbiditaacutes bull deafferentaacutecioacutes faacutejdalmak kialakulaacutesa
Funkcionaacutelis idegsebeacuteszetdefiniacutecioacute
bull Koacuteros idegrendszeri műkoumldeacutesek (funkcioacutek) műteacuteti uacuteton toumlrteacutenő befolyaacutesolaacutesa (normalizaacutelaacutesa)
Funkcionaacutelis idegsebeacuteszet -alkalmazaacutesi teruumlletek
bull kroacutenikus faacutejdalom
bull mozgaacuteszavarok
bull spasticitaacutes
bull epilepszia
bull psychochirurgia
bull vegetatiacutev zavarok
Neuromodulaacutecioacute
bull centraacutelis-perifeacuteriaacutes-autonom idegrendszer műkoumldeacuteseacutenek teraacutepiaacutes alteraacutecioacuteja
bull implantaacutelt keacuteszuumlleacutek
bull elektromos gyoacutegyszeres
bull non-destruktiacutev
bull reverzibilis
bull betegseacuteget nem gyoacutegyiacutet
bull műkoumldeacutest eacuteletminőseacuteget javiacutet
Neuromodulaacutecioacute tiacutepusai
bull Elektromos (neurostimulaacutecioacute)
bull Keacutemiai (gyoacutegyszerpumpa)
Neuropathic pain
bull International Association for the Study of Pain defines pain caused by a lesion or disease of the somatosensory nervous system
bull suffer more often from insomnia anxiety and depression1
bull analgetic medication insufficient2
bull SCS has undergone constant technical advancement
Why Neuromodulation
bull Testable
bull Completely reversible
bull Non-destructive
bull No limitation to future therapy
Neurostimulaacutecioacute helye
bull perifeacuteriaacutes ideg PNS PNfS DRGS
bull gerincvelő SCS
bull meacutelyagyi DBS
bull motoros agykeacutereg MCS
Neurostimulaacutecioacutes faacutejdalomcsillapiacutetoacute műteacutetek indikaacutecioacutejaacutenak felaacutelliacutetaacutesa
bull faacutejdalom kezeleacuteseacuteben jaacuteratos szakemberek koumlzoumls doumlnteacutese
bull centrumokban (kivizsgaacutelaacutes kezeleacutes szoumlvődmeacutenyek elhaacuteriacutetaacutesa)
bull multidisciplinaacuteris (ideggyoacutegyaacutesz idegsebeacutesz psychiaacuteter psycholoacutegus anaesthesioloacutegus neuroradioloacutegus elektrofizioloacutegus mozgaacutesterapeuta) munkacsoport
Neurostimulaacutecioacute aacuteltalaacutenos kontraindikaacutecioacutek
(kroacutenikus faacutejdalom)
bull psychiaacutetriai koacuterkeacutepek (aktiacutev psychosis suacutelyos depresszioacute hipochondria szomatizaacutecioacutes betegseacutegek)
bull nem egyuumlttműkoumldő beteg
bull alkoholizmus kaacutebiacutetoacuteszer-eacutelvezet
bull suacutelyos kiacuteseacuterő betegseacuteg (coagulopathia immundeficiencia)
bull maacutes implantaacutelt pacemaker (pl sziacutev)
Neurostimulaacutecioacute műteacuteti szoumlvődmeacutenyek
bull korrigaacutelhatoacutek
bull implantaacutetummal (8-10) kapcsolatos
(elektroacuteda elmozdulaacutes seacuteruumlleacutes elektromos műkoumldeacutes zavar)
bull veacuterzeacutesek (1-5)
bull gyulladaacutesok (5-7)
Spinal cord stimulaacutecioacute (SCS)
bull Legneacutepszerűbb leggyakrabban alkalmazott
bull Első SCS daganatos faacutejdalom (Shealey 1967)
History of Spinal Cord StimulationShealy 1969
bull 1967 ndash Long and Wall PNS
bull 1969 ndash Shealy SCS in humans
bull 1975 ndash Dooley perc electrode
bull Mid 1970s ndash self-powered battery
bull 1980s - programmable quad electrode
bull 1980s -1990s ndash Primary cell IPG
bull 2004 ndash Rechargeable IPG
Clinical studies on SCS continue to support the effectiveness of this
therapy The following charts summarize studies of SCS and its
effects on the quality of life of patients
Reduction of Pain
ReferenceNumber of
PatientsFollow Up Results
Kumar17 410 8 years 74 had gt50 relief
North14 19 3 years 47 had gt50 relief
Barolat9 41 1 year50-65 had good to
excellent relief
Van Buyten18 123 3 years68 had good to excellent
relief
Cameron19 747Up to 59 months
(49 years)
62 had gt50 relief or
significantly reduced pain
scores
SCS indikaacutecioacutek INeuropaacutethiaacutes (neurogeacuten) faacutejdalom
bull Perifeacuteriaacutes idegek seacuteruumlleacutese gyoumlkoumlk plexusok (idegrendszeri hiaacutenytuumlnet) seacuteruumlleacutes okai baleseti műteacutet pl lumbaacutelis discectomia (gyoumlk) nőgyoacutegyaacuteszati (inguinalis ideg) teacuterdműteacutetek (infrapatellaacuteris ideg) mastectomia (costo-brachiaacutelis ideg)
bull veacutegtag-amputaacutecioacute csonkfaacutejdalom jobban mint a fantom faacutejdalombull post-herpeses neuralgia amennyiben a bőreacuterzeacutes reacuteszlegesen megtartottbull post-irradiaacutecioacutes plexopaacutetiabull polyneuropaacutetiaacutek (diabeteses alkoholos) post-kemoteraacutepiaacutes (amennyiben a vastag rostok
műkoumldeacutese reacuteszlegesen megtartott)bull gerincvelő incomplett seacuteruumlleacutese -amennyiben a vastag eacuterzőrostok műkoumldeacutese megtartott eacutes a
segmentaacutelis faacutejdalom a seacuteruumlleacutes magassaacutegaacuteban leacutep felbull cervicaacutelis eacutes lumbosacralis radiculopaacutetiaacutek (compresszioacute ischaemia sebeacuteszi baleset
arachnoiditisbull CRPS II (causalga)bull DE bull plexus avulsioacute syringomyelia faacutejdalom nem csillapiacutethatoacutek bull nincs egyeteacuterteacutes a CRPS I (reflex sympaticus dystrophia)
SCS indikaacutecioacutek II
bull Kevert faacutejdalom szindroacutemaacutek
Falied back surgery syndroma = FBSS koraacutebbi gerincsebeacuteszeti beavatkozaacutes (postoperatiacutev fibrosis arachnoiditis)
Posztlaminektomiaacutes szindroacutemaangolszaacutesz failed back surgery szindroacutemaacutenak (FBSS)
bull faacutejdalom lokalizaacutecioacute alsoacute aacutegyeacuteki gerinc far
alsoacute veacutegtagok
bull etioloacutegia arachnoiditis epiduraacutelis heg
radiculitis mikro-instabilitaacutes rec
porckorongseacuterv gyulladaacutes
bull tapasztalatok alsoacute veacutegtagba terjedő
faacutejdalomra SCS hateacutekony
bull axiaacutelis faacutejdalmakra nem bizonyiacutetott
Incidencia FBSS
bull ranges 5 - 50
bull postdiscectomy 10-40
Etiologia FBSS
bull Scar tissue that forms around the surgery site interrupting normal neurological functioning
bull technicalities of the operation are not successful the performing surgeon had poor technique andor there is iatrogenic injury present
bull surgery is not performed at the site that causes the pain
bull surgery performed is not actually necessarybull patient is a poor fit for a successful surgerybull diagnosis was incorrectbull Complications of surgery arise
1 Anderson VC et al Current review of pain 20004105-11 5 Vaccaro AR et al Spine 200126 (24) S111-82 Leveque JC et al Neuromodulation 200141-9 6 Spengler DM et al Spine 19805356-603 Dario A et al Neuromodulation 20014105-110 7 Fager CA Freidberg SR Spine 1980587-944 Ohnmeiss DD et al The Spine Journal 2001358-363 8 Long DM Surgical management of pain 2002 354-64
FBSS okai eacutes tuumlnetei
bull FBSS cause1-7
ndash irreversible nerve injury
ndash surgical complications
ndash psychosocial problems
ndash inappropriate selection of patients for surgery
ndash recurrent herniation
ndash wrong level of operation
bull FBSS symptoms348
ndash lumbosacral postoperative fibrosis andor arachnoiditis
ndash root lesion
ndash dorsal compartment syndrome
ndash lateral spinal stenosis
SCS indikaacutecioacutek IIIAngina pectoris
bull New York Heart Association III-IV csoport (szignifikaacutens coronaacuteria stenosis egy vagy toumlbb szűkuumllet 70 )
bull myocardiaacutelis ischaemia reverzibilis angina gyoacutegyszeres revascularizaacutecioacutes beavatkozaacutesokkal nem enyhiacutethető
bull eacuteletminőseacuteguarr nitro-glicerin felhasznaacutelaacutesdarr anginaacutes rohamok szaacutemadarr jaacuteraacutestaacutevolsaacuteguarr
bull SCS anti-ischaemiaacutes hataacutes
bull nincs bizonyiacuteteacutek SCS hateacutekonysaacutegra instabil angina acut myocardiaacutelis infarctus vazospasticus angia maacutes sziacutevbetegseacuteg okozta anginaacutes faacutejdalmak csillapiacutetaacutesaacutera
Anginaacutes faacutejdalom
SCS tanulmaacutenyok hateacutekonysaacuteg I
bull Nienke (45 ) PT 1 eacutev koumlveteacutes eacuteletminőseacuteg szociaacutelis mentaacutelis fizikaacutelis teljesiacutetmeacuteny szignifikaacutensan javul
bull Hautvast (46) stabil angina pectorisban RT 6 heacutet koumlveteacutes
Randomizaacutelaacutes a stimulaacutetor OFF b csoport 3x1 oacuteranap ON vagy hirtelen anginaacuteban
anginaacutes rohamszaacutem csoumlkken
fizikai teljesiacutetőkeacutepesseacuteg javul
sublinguaacutelis nitraacutet felhasznaacutelaacutes csoumlkken
EKG-n az ischaemiaacutes epizoacutedusok csoumlkkennek
ST depresszioacute enyhuumll eacuteletminőseacuteg javul
anginaacutes faacutejdalom csoumlkken
SCS indikaacutecioacutek IIIAngina pectoris
bull tanulmaacutenyok eredmeacutenyei kedvezőek (39-43)
bull teraacutepiaacutes hataacutes hosszuacute taacutevuacute
bull nitraacutet bevitel csoumlkkenthető
bull faacutejdalomcsillapiacutetoacute hataacutesuacute
bull sziacutevizom veacuterkeringeacutes javul
bull PET tanulmaacuteny
ischaemiaacutes sziacutevizomban keringeacuteseacuteben
redistribucio alakul ki nyugalomban
eacutes gyoacutegyszer indukaacutelt stresszben(44)
SCS indikaacutecioacutek IVPerifeacuteriaacutes vasculaacuteris betegseacutegek
bull lassan progrediaacuteloacute perifeacuteriaacutes vasculaacuteris ischaemia -atherosclerosis (Fontaine 3 4 staacutedium )
bull vazospasticus betegseacuteg (pl Raynaud frostbite) gyoacutegyszeresen eacutersebeacuteszeti műteacutettel nem uralhatoacute veacutegtagfaacutejdalom
bull Buerger-koacuter
bull kontraindikaacutelt laacutebszaacuterfekeacutelygt 3 cm gangreacutena
SCS indikaacutecioacutek VCRPS
CRPS tuumlnetei
1 Harden RN et al Pain 199983211-219 6Birklein F et al Pain 19976949-54
2 Galer BS et al J Pain Symptom Manage 200020286-92 7 Schwartzman RJ Kerrigan J
Neurosurgery 19904057-61
3 Birklein F Handwerker HO Pain 2001 941-6 8 Zyluk A J Hand Surg 200126151-154
4 Rommel O et al Pain 19998095-101 9 Wasner G et al Neuro Clin
199816851-68
5 Thimineur M et al Clin J Pain 199814256-67
Sensory Motor dysfunctionIntense pain12 Weakness
Allodynia13 Decreased range of motion3
Hyperesthesia13 Tremor16
Hyperalgesia13 Dystonia7
Sensory deficits4 Myoclonus7
Decreased muscular strength8
Autonomic Dystrophic Swelling1 Increaseddecreased nailhair growth
Colourtemperature changes6 Skin changes (eg palor plantar fibrosis
Sweating abnormalities6 hyperkeratosis and thin glossy
skin9 )
Courtesy of Robert J Schwartzman MD
SCS indikaacutecioacutek VIAbdominaacutelis eacutes visceraacutelis faacutejdalom
szindroacutemaacutek
bull Faacutejdalom etioloacutegiaacuteja vaacuteltozatos
bull Ok gastrointestinaacutelis gastro-urinaacutelis
musculosceletaacutelis idegrendszeri
bull Megfigyeleacutes Th X myelotomia
daganatos pelvicus faacutejdalmat csillapiacutet
Mechanisms of SCS
bull Gate control theory
bull Direct inhibition of spinothalamic neurons
bull Descending modulatory effects
bull Alteration of sympathetic activity
bull Neurochemical modulation
GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Neuropathiaacutes neurogeacuten faacutejdalom
bull Idegrendszeri seacuteruumlleacutes (eacuterzőpaacutelya) koumlvetkezmeacutenye
bull Idegrendszeri tuumlnet
bull Faacutejdalomvezető paacutelyaacutek innervaacutecioacutejaacutenakelveszteacutese
bull Eacutegő eacuterzeacuteszavar
bull Nem reagaacutel opiaacutetokra
Neuropathiaacutes neurogeacuten faacutejdalomjellemzői
bull Thermaacutelis (eacutegő hideg)
bull exteroceptiv (elektromos villaacutemlaacutesszerűcsiacutepő szuacuteroacute)
dysaesthesia
bull Proprioceptiv (szaggatoacute szoriacutetoacute markoloacute)
aacutellandoacute időszakos kuumllső ingerekkel kivaacutelthatoacute (thermaacutelis tactilis proprioceptiv allodynia hyperalgeacutezia)
Idegsebeacuteszeti faacutejdalomcsillapiacutetaacutesi lehetőseacutegek neuropaacutetiaacutes faacutejdalomban
bull Ablatiacutev
bull Neuromodulaacutecioacute
Ablatiacutev faacutejdalomcsillapiacutetoacute idegsebeacuteszeti beavatkozaacutesok
bull faacutejdalomvezető paacutelyaacutekat aacutetmetszeacutese roncsolaacutesa destruktiacutev (rizotomiaDREZmyelotomiatermocoagulaacutecioacute)
bull szaacutemos esetben hataacutestalan bull hataacutes aacutetmenetibull maradandoacute hiaacutenytuumlnetbull irreverzibilis magasabb morbiditaacutes bull deafferentaacutecioacutes faacutejdalmak kialakulaacutesa
Funkcionaacutelis idegsebeacuteszetdefiniacutecioacute
bull Koacuteros idegrendszeri műkoumldeacutesek (funkcioacutek) műteacuteti uacuteton toumlrteacutenő befolyaacutesolaacutesa (normalizaacutelaacutesa)
Funkcionaacutelis idegsebeacuteszet -alkalmazaacutesi teruumlletek
bull kroacutenikus faacutejdalom
bull mozgaacuteszavarok
bull spasticitaacutes
bull epilepszia
bull psychochirurgia
bull vegetatiacutev zavarok
Neuromodulaacutecioacute
bull centraacutelis-perifeacuteriaacutes-autonom idegrendszer műkoumldeacuteseacutenek teraacutepiaacutes alteraacutecioacuteja
bull implantaacutelt keacuteszuumlleacutek
bull elektromos gyoacutegyszeres
bull non-destruktiacutev
bull reverzibilis
bull betegseacuteget nem gyoacutegyiacutet
bull műkoumldeacutest eacuteletminőseacuteget javiacutet
Neuromodulaacutecioacute tiacutepusai
bull Elektromos (neurostimulaacutecioacute)
bull Keacutemiai (gyoacutegyszerpumpa)
Neuropathic pain
bull International Association for the Study of Pain defines pain caused by a lesion or disease of the somatosensory nervous system
bull suffer more often from insomnia anxiety and depression1
bull analgetic medication insufficient2
bull SCS has undergone constant technical advancement
Why Neuromodulation
bull Testable
bull Completely reversible
bull Non-destructive
bull No limitation to future therapy
Neurostimulaacutecioacute helye
bull perifeacuteriaacutes ideg PNS PNfS DRGS
bull gerincvelő SCS
bull meacutelyagyi DBS
bull motoros agykeacutereg MCS
Neurostimulaacutecioacutes faacutejdalomcsillapiacutetoacute műteacutetek indikaacutecioacutejaacutenak felaacutelliacutetaacutesa
bull faacutejdalom kezeleacuteseacuteben jaacuteratos szakemberek koumlzoumls doumlnteacutese
bull centrumokban (kivizsgaacutelaacutes kezeleacutes szoumlvődmeacutenyek elhaacuteriacutetaacutesa)
bull multidisciplinaacuteris (ideggyoacutegyaacutesz idegsebeacutesz psychiaacuteter psycholoacutegus anaesthesioloacutegus neuroradioloacutegus elektrofizioloacutegus mozgaacutesterapeuta) munkacsoport
Neurostimulaacutecioacute aacuteltalaacutenos kontraindikaacutecioacutek
(kroacutenikus faacutejdalom)
bull psychiaacutetriai koacuterkeacutepek (aktiacutev psychosis suacutelyos depresszioacute hipochondria szomatizaacutecioacutes betegseacutegek)
bull nem egyuumlttműkoumldő beteg
bull alkoholizmus kaacutebiacutetoacuteszer-eacutelvezet
bull suacutelyos kiacuteseacuterő betegseacuteg (coagulopathia immundeficiencia)
bull maacutes implantaacutelt pacemaker (pl sziacutev)
Neurostimulaacutecioacute műteacuteti szoumlvődmeacutenyek
bull korrigaacutelhatoacutek
bull implantaacutetummal (8-10) kapcsolatos
(elektroacuteda elmozdulaacutes seacuteruumlleacutes elektromos műkoumldeacutes zavar)
bull veacuterzeacutesek (1-5)
bull gyulladaacutesok (5-7)
Spinal cord stimulaacutecioacute (SCS)
bull Legneacutepszerűbb leggyakrabban alkalmazott
bull Első SCS daganatos faacutejdalom (Shealey 1967)
History of Spinal Cord StimulationShealy 1969
bull 1967 ndash Long and Wall PNS
bull 1969 ndash Shealy SCS in humans
bull 1975 ndash Dooley perc electrode
bull Mid 1970s ndash self-powered battery
bull 1980s - programmable quad electrode
bull 1980s -1990s ndash Primary cell IPG
bull 2004 ndash Rechargeable IPG
Clinical studies on SCS continue to support the effectiveness of this
therapy The following charts summarize studies of SCS and its
effects on the quality of life of patients
Reduction of Pain
ReferenceNumber of
PatientsFollow Up Results
Kumar17 410 8 years 74 had gt50 relief
North14 19 3 years 47 had gt50 relief
Barolat9 41 1 year50-65 had good to
excellent relief
Van Buyten18 123 3 years68 had good to excellent
relief
Cameron19 747Up to 59 months
(49 years)
62 had gt50 relief or
significantly reduced pain
scores
SCS indikaacutecioacutek INeuropaacutethiaacutes (neurogeacuten) faacutejdalom
bull Perifeacuteriaacutes idegek seacuteruumlleacutese gyoumlkoumlk plexusok (idegrendszeri hiaacutenytuumlnet) seacuteruumlleacutes okai baleseti műteacutet pl lumbaacutelis discectomia (gyoumlk) nőgyoacutegyaacuteszati (inguinalis ideg) teacuterdműteacutetek (infrapatellaacuteris ideg) mastectomia (costo-brachiaacutelis ideg)
bull veacutegtag-amputaacutecioacute csonkfaacutejdalom jobban mint a fantom faacutejdalombull post-herpeses neuralgia amennyiben a bőreacuterzeacutes reacuteszlegesen megtartottbull post-irradiaacutecioacutes plexopaacutetiabull polyneuropaacutetiaacutek (diabeteses alkoholos) post-kemoteraacutepiaacutes (amennyiben a vastag rostok
műkoumldeacutese reacuteszlegesen megtartott)bull gerincvelő incomplett seacuteruumlleacutese -amennyiben a vastag eacuterzőrostok műkoumldeacutese megtartott eacutes a
segmentaacutelis faacutejdalom a seacuteruumlleacutes magassaacutegaacuteban leacutep felbull cervicaacutelis eacutes lumbosacralis radiculopaacutetiaacutek (compresszioacute ischaemia sebeacuteszi baleset
arachnoiditisbull CRPS II (causalga)bull DE bull plexus avulsioacute syringomyelia faacutejdalom nem csillapiacutethatoacutek bull nincs egyeteacuterteacutes a CRPS I (reflex sympaticus dystrophia)
SCS indikaacutecioacutek II
bull Kevert faacutejdalom szindroacutemaacutek
Falied back surgery syndroma = FBSS koraacutebbi gerincsebeacuteszeti beavatkozaacutes (postoperatiacutev fibrosis arachnoiditis)
Posztlaminektomiaacutes szindroacutemaangolszaacutesz failed back surgery szindroacutemaacutenak (FBSS)
bull faacutejdalom lokalizaacutecioacute alsoacute aacutegyeacuteki gerinc far
alsoacute veacutegtagok
bull etioloacutegia arachnoiditis epiduraacutelis heg
radiculitis mikro-instabilitaacutes rec
porckorongseacuterv gyulladaacutes
bull tapasztalatok alsoacute veacutegtagba terjedő
faacutejdalomra SCS hateacutekony
bull axiaacutelis faacutejdalmakra nem bizonyiacutetott
Incidencia FBSS
bull ranges 5 - 50
bull postdiscectomy 10-40
Etiologia FBSS
bull Scar tissue that forms around the surgery site interrupting normal neurological functioning
bull technicalities of the operation are not successful the performing surgeon had poor technique andor there is iatrogenic injury present
bull surgery is not performed at the site that causes the pain
bull surgery performed is not actually necessarybull patient is a poor fit for a successful surgerybull diagnosis was incorrectbull Complications of surgery arise
1 Anderson VC et al Current review of pain 20004105-11 5 Vaccaro AR et al Spine 200126 (24) S111-82 Leveque JC et al Neuromodulation 200141-9 6 Spengler DM et al Spine 19805356-603 Dario A et al Neuromodulation 20014105-110 7 Fager CA Freidberg SR Spine 1980587-944 Ohnmeiss DD et al The Spine Journal 2001358-363 8 Long DM Surgical management of pain 2002 354-64
FBSS okai eacutes tuumlnetei
bull FBSS cause1-7
ndash irreversible nerve injury
ndash surgical complications
ndash psychosocial problems
ndash inappropriate selection of patients for surgery
ndash recurrent herniation
ndash wrong level of operation
bull FBSS symptoms348
ndash lumbosacral postoperative fibrosis andor arachnoiditis
ndash root lesion
ndash dorsal compartment syndrome
ndash lateral spinal stenosis
SCS indikaacutecioacutek IIIAngina pectoris
bull New York Heart Association III-IV csoport (szignifikaacutens coronaacuteria stenosis egy vagy toumlbb szűkuumllet 70 )
bull myocardiaacutelis ischaemia reverzibilis angina gyoacutegyszeres revascularizaacutecioacutes beavatkozaacutesokkal nem enyhiacutethető
bull eacuteletminőseacuteguarr nitro-glicerin felhasznaacutelaacutesdarr anginaacutes rohamok szaacutemadarr jaacuteraacutestaacutevolsaacuteguarr
bull SCS anti-ischaemiaacutes hataacutes
bull nincs bizonyiacuteteacutek SCS hateacutekonysaacutegra instabil angina acut myocardiaacutelis infarctus vazospasticus angia maacutes sziacutevbetegseacuteg okozta anginaacutes faacutejdalmak csillapiacutetaacutesaacutera
Anginaacutes faacutejdalom
SCS tanulmaacutenyok hateacutekonysaacuteg I
bull Nienke (45 ) PT 1 eacutev koumlveteacutes eacuteletminőseacuteg szociaacutelis mentaacutelis fizikaacutelis teljesiacutetmeacuteny szignifikaacutensan javul
bull Hautvast (46) stabil angina pectorisban RT 6 heacutet koumlveteacutes
Randomizaacutelaacutes a stimulaacutetor OFF b csoport 3x1 oacuteranap ON vagy hirtelen anginaacuteban
anginaacutes rohamszaacutem csoumlkken
fizikai teljesiacutetőkeacutepesseacuteg javul
sublinguaacutelis nitraacutet felhasznaacutelaacutes csoumlkken
EKG-n az ischaemiaacutes epizoacutedusok csoumlkkennek
ST depresszioacute enyhuumll eacuteletminőseacuteg javul
anginaacutes faacutejdalom csoumlkken
SCS indikaacutecioacutek IIIAngina pectoris
bull tanulmaacutenyok eredmeacutenyei kedvezőek (39-43)
bull teraacutepiaacutes hataacutes hosszuacute taacutevuacute
bull nitraacutet bevitel csoumlkkenthető
bull faacutejdalomcsillapiacutetoacute hataacutesuacute
bull sziacutevizom veacuterkeringeacutes javul
bull PET tanulmaacuteny
ischaemiaacutes sziacutevizomban keringeacuteseacuteben
redistribucio alakul ki nyugalomban
eacutes gyoacutegyszer indukaacutelt stresszben(44)
SCS indikaacutecioacutek IVPerifeacuteriaacutes vasculaacuteris betegseacutegek
bull lassan progrediaacuteloacute perifeacuteriaacutes vasculaacuteris ischaemia -atherosclerosis (Fontaine 3 4 staacutedium )
bull vazospasticus betegseacuteg (pl Raynaud frostbite) gyoacutegyszeresen eacutersebeacuteszeti műteacutettel nem uralhatoacute veacutegtagfaacutejdalom
bull Buerger-koacuter
bull kontraindikaacutelt laacutebszaacuterfekeacutelygt 3 cm gangreacutena
SCS indikaacutecioacutek VCRPS
CRPS tuumlnetei
1 Harden RN et al Pain 199983211-219 6Birklein F et al Pain 19976949-54
2 Galer BS et al J Pain Symptom Manage 200020286-92 7 Schwartzman RJ Kerrigan J
Neurosurgery 19904057-61
3 Birklein F Handwerker HO Pain 2001 941-6 8 Zyluk A J Hand Surg 200126151-154
4 Rommel O et al Pain 19998095-101 9 Wasner G et al Neuro Clin
199816851-68
5 Thimineur M et al Clin J Pain 199814256-67
Sensory Motor dysfunctionIntense pain12 Weakness
Allodynia13 Decreased range of motion3
Hyperesthesia13 Tremor16
Hyperalgesia13 Dystonia7
Sensory deficits4 Myoclonus7
Decreased muscular strength8
Autonomic Dystrophic Swelling1 Increaseddecreased nailhair growth
Colourtemperature changes6 Skin changes (eg palor plantar fibrosis
Sweating abnormalities6 hyperkeratosis and thin glossy
skin9 )
Courtesy of Robert J Schwartzman MD
SCS indikaacutecioacutek VIAbdominaacutelis eacutes visceraacutelis faacutejdalom
szindroacutemaacutek
bull Faacutejdalom etioloacutegiaacuteja vaacuteltozatos
bull Ok gastrointestinaacutelis gastro-urinaacutelis
musculosceletaacutelis idegrendszeri
bull Megfigyeleacutes Th X myelotomia
daganatos pelvicus faacutejdalmat csillapiacutet
Mechanisms of SCS
bull Gate control theory
bull Direct inhibition of spinothalamic neurons
bull Descending modulatory effects
bull Alteration of sympathetic activity
bull Neurochemical modulation
GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Neuropathiaacutes neurogeacuten faacutejdalomjellemzői
bull Thermaacutelis (eacutegő hideg)
bull exteroceptiv (elektromos villaacutemlaacutesszerűcsiacutepő szuacuteroacute)
dysaesthesia
bull Proprioceptiv (szaggatoacute szoriacutetoacute markoloacute)
aacutellandoacute időszakos kuumllső ingerekkel kivaacutelthatoacute (thermaacutelis tactilis proprioceptiv allodynia hyperalgeacutezia)
Idegsebeacuteszeti faacutejdalomcsillapiacutetaacutesi lehetőseacutegek neuropaacutetiaacutes faacutejdalomban
bull Ablatiacutev
bull Neuromodulaacutecioacute
Ablatiacutev faacutejdalomcsillapiacutetoacute idegsebeacuteszeti beavatkozaacutesok
bull faacutejdalomvezető paacutelyaacutekat aacutetmetszeacutese roncsolaacutesa destruktiacutev (rizotomiaDREZmyelotomiatermocoagulaacutecioacute)
bull szaacutemos esetben hataacutestalan bull hataacutes aacutetmenetibull maradandoacute hiaacutenytuumlnetbull irreverzibilis magasabb morbiditaacutes bull deafferentaacutecioacutes faacutejdalmak kialakulaacutesa
Funkcionaacutelis idegsebeacuteszetdefiniacutecioacute
bull Koacuteros idegrendszeri műkoumldeacutesek (funkcioacutek) műteacuteti uacuteton toumlrteacutenő befolyaacutesolaacutesa (normalizaacutelaacutesa)
Funkcionaacutelis idegsebeacuteszet -alkalmazaacutesi teruumlletek
bull kroacutenikus faacutejdalom
bull mozgaacuteszavarok
bull spasticitaacutes
bull epilepszia
bull psychochirurgia
bull vegetatiacutev zavarok
Neuromodulaacutecioacute
bull centraacutelis-perifeacuteriaacutes-autonom idegrendszer műkoumldeacuteseacutenek teraacutepiaacutes alteraacutecioacuteja
bull implantaacutelt keacuteszuumlleacutek
bull elektromos gyoacutegyszeres
bull non-destruktiacutev
bull reverzibilis
bull betegseacuteget nem gyoacutegyiacutet
bull műkoumldeacutest eacuteletminőseacuteget javiacutet
Neuromodulaacutecioacute tiacutepusai
bull Elektromos (neurostimulaacutecioacute)
bull Keacutemiai (gyoacutegyszerpumpa)
Neuropathic pain
bull International Association for the Study of Pain defines pain caused by a lesion or disease of the somatosensory nervous system
bull suffer more often from insomnia anxiety and depression1
bull analgetic medication insufficient2
bull SCS has undergone constant technical advancement
Why Neuromodulation
bull Testable
bull Completely reversible
bull Non-destructive
bull No limitation to future therapy
Neurostimulaacutecioacute helye
bull perifeacuteriaacutes ideg PNS PNfS DRGS
bull gerincvelő SCS
bull meacutelyagyi DBS
bull motoros agykeacutereg MCS
Neurostimulaacutecioacutes faacutejdalomcsillapiacutetoacute műteacutetek indikaacutecioacutejaacutenak felaacutelliacutetaacutesa
bull faacutejdalom kezeleacuteseacuteben jaacuteratos szakemberek koumlzoumls doumlnteacutese
bull centrumokban (kivizsgaacutelaacutes kezeleacutes szoumlvődmeacutenyek elhaacuteriacutetaacutesa)
bull multidisciplinaacuteris (ideggyoacutegyaacutesz idegsebeacutesz psychiaacuteter psycholoacutegus anaesthesioloacutegus neuroradioloacutegus elektrofizioloacutegus mozgaacutesterapeuta) munkacsoport
Neurostimulaacutecioacute aacuteltalaacutenos kontraindikaacutecioacutek
(kroacutenikus faacutejdalom)
bull psychiaacutetriai koacuterkeacutepek (aktiacutev psychosis suacutelyos depresszioacute hipochondria szomatizaacutecioacutes betegseacutegek)
bull nem egyuumlttműkoumldő beteg
bull alkoholizmus kaacutebiacutetoacuteszer-eacutelvezet
bull suacutelyos kiacuteseacuterő betegseacuteg (coagulopathia immundeficiencia)
bull maacutes implantaacutelt pacemaker (pl sziacutev)
Neurostimulaacutecioacute műteacuteti szoumlvődmeacutenyek
bull korrigaacutelhatoacutek
bull implantaacutetummal (8-10) kapcsolatos
(elektroacuteda elmozdulaacutes seacuteruumlleacutes elektromos műkoumldeacutes zavar)
bull veacuterzeacutesek (1-5)
bull gyulladaacutesok (5-7)
Spinal cord stimulaacutecioacute (SCS)
bull Legneacutepszerűbb leggyakrabban alkalmazott
bull Első SCS daganatos faacutejdalom (Shealey 1967)
History of Spinal Cord StimulationShealy 1969
bull 1967 ndash Long and Wall PNS
bull 1969 ndash Shealy SCS in humans
bull 1975 ndash Dooley perc electrode
bull Mid 1970s ndash self-powered battery
bull 1980s - programmable quad electrode
bull 1980s -1990s ndash Primary cell IPG
bull 2004 ndash Rechargeable IPG
Clinical studies on SCS continue to support the effectiveness of this
therapy The following charts summarize studies of SCS and its
effects on the quality of life of patients
Reduction of Pain
ReferenceNumber of
PatientsFollow Up Results
Kumar17 410 8 years 74 had gt50 relief
North14 19 3 years 47 had gt50 relief
Barolat9 41 1 year50-65 had good to
excellent relief
Van Buyten18 123 3 years68 had good to excellent
relief
Cameron19 747Up to 59 months
(49 years)
62 had gt50 relief or
significantly reduced pain
scores
SCS indikaacutecioacutek INeuropaacutethiaacutes (neurogeacuten) faacutejdalom
bull Perifeacuteriaacutes idegek seacuteruumlleacutese gyoumlkoumlk plexusok (idegrendszeri hiaacutenytuumlnet) seacuteruumlleacutes okai baleseti műteacutet pl lumbaacutelis discectomia (gyoumlk) nőgyoacutegyaacuteszati (inguinalis ideg) teacuterdműteacutetek (infrapatellaacuteris ideg) mastectomia (costo-brachiaacutelis ideg)
bull veacutegtag-amputaacutecioacute csonkfaacutejdalom jobban mint a fantom faacutejdalombull post-herpeses neuralgia amennyiben a bőreacuterzeacutes reacuteszlegesen megtartottbull post-irradiaacutecioacutes plexopaacutetiabull polyneuropaacutetiaacutek (diabeteses alkoholos) post-kemoteraacutepiaacutes (amennyiben a vastag rostok
műkoumldeacutese reacuteszlegesen megtartott)bull gerincvelő incomplett seacuteruumlleacutese -amennyiben a vastag eacuterzőrostok műkoumldeacutese megtartott eacutes a
segmentaacutelis faacutejdalom a seacuteruumlleacutes magassaacutegaacuteban leacutep felbull cervicaacutelis eacutes lumbosacralis radiculopaacutetiaacutek (compresszioacute ischaemia sebeacuteszi baleset
arachnoiditisbull CRPS II (causalga)bull DE bull plexus avulsioacute syringomyelia faacutejdalom nem csillapiacutethatoacutek bull nincs egyeteacuterteacutes a CRPS I (reflex sympaticus dystrophia)
SCS indikaacutecioacutek II
bull Kevert faacutejdalom szindroacutemaacutek
Falied back surgery syndroma = FBSS koraacutebbi gerincsebeacuteszeti beavatkozaacutes (postoperatiacutev fibrosis arachnoiditis)
Posztlaminektomiaacutes szindroacutemaangolszaacutesz failed back surgery szindroacutemaacutenak (FBSS)
bull faacutejdalom lokalizaacutecioacute alsoacute aacutegyeacuteki gerinc far
alsoacute veacutegtagok
bull etioloacutegia arachnoiditis epiduraacutelis heg
radiculitis mikro-instabilitaacutes rec
porckorongseacuterv gyulladaacutes
bull tapasztalatok alsoacute veacutegtagba terjedő
faacutejdalomra SCS hateacutekony
bull axiaacutelis faacutejdalmakra nem bizonyiacutetott
Incidencia FBSS
bull ranges 5 - 50
bull postdiscectomy 10-40
Etiologia FBSS
bull Scar tissue that forms around the surgery site interrupting normal neurological functioning
bull technicalities of the operation are not successful the performing surgeon had poor technique andor there is iatrogenic injury present
bull surgery is not performed at the site that causes the pain
bull surgery performed is not actually necessarybull patient is a poor fit for a successful surgerybull diagnosis was incorrectbull Complications of surgery arise
1 Anderson VC et al Current review of pain 20004105-11 5 Vaccaro AR et al Spine 200126 (24) S111-82 Leveque JC et al Neuromodulation 200141-9 6 Spengler DM et al Spine 19805356-603 Dario A et al Neuromodulation 20014105-110 7 Fager CA Freidberg SR Spine 1980587-944 Ohnmeiss DD et al The Spine Journal 2001358-363 8 Long DM Surgical management of pain 2002 354-64
FBSS okai eacutes tuumlnetei
bull FBSS cause1-7
ndash irreversible nerve injury
ndash surgical complications
ndash psychosocial problems
ndash inappropriate selection of patients for surgery
ndash recurrent herniation
ndash wrong level of operation
bull FBSS symptoms348
ndash lumbosacral postoperative fibrosis andor arachnoiditis
ndash root lesion
ndash dorsal compartment syndrome
ndash lateral spinal stenosis
SCS indikaacutecioacutek IIIAngina pectoris
bull New York Heart Association III-IV csoport (szignifikaacutens coronaacuteria stenosis egy vagy toumlbb szűkuumllet 70 )
bull myocardiaacutelis ischaemia reverzibilis angina gyoacutegyszeres revascularizaacutecioacutes beavatkozaacutesokkal nem enyhiacutethető
bull eacuteletminőseacuteguarr nitro-glicerin felhasznaacutelaacutesdarr anginaacutes rohamok szaacutemadarr jaacuteraacutestaacutevolsaacuteguarr
bull SCS anti-ischaemiaacutes hataacutes
bull nincs bizonyiacuteteacutek SCS hateacutekonysaacutegra instabil angina acut myocardiaacutelis infarctus vazospasticus angia maacutes sziacutevbetegseacuteg okozta anginaacutes faacutejdalmak csillapiacutetaacutesaacutera
Anginaacutes faacutejdalom
SCS tanulmaacutenyok hateacutekonysaacuteg I
bull Nienke (45 ) PT 1 eacutev koumlveteacutes eacuteletminőseacuteg szociaacutelis mentaacutelis fizikaacutelis teljesiacutetmeacuteny szignifikaacutensan javul
bull Hautvast (46) stabil angina pectorisban RT 6 heacutet koumlveteacutes
Randomizaacutelaacutes a stimulaacutetor OFF b csoport 3x1 oacuteranap ON vagy hirtelen anginaacuteban
anginaacutes rohamszaacutem csoumlkken
fizikai teljesiacutetőkeacutepesseacuteg javul
sublinguaacutelis nitraacutet felhasznaacutelaacutes csoumlkken
EKG-n az ischaemiaacutes epizoacutedusok csoumlkkennek
ST depresszioacute enyhuumll eacuteletminőseacuteg javul
anginaacutes faacutejdalom csoumlkken
SCS indikaacutecioacutek IIIAngina pectoris
bull tanulmaacutenyok eredmeacutenyei kedvezőek (39-43)
bull teraacutepiaacutes hataacutes hosszuacute taacutevuacute
bull nitraacutet bevitel csoumlkkenthető
bull faacutejdalomcsillapiacutetoacute hataacutesuacute
bull sziacutevizom veacuterkeringeacutes javul
bull PET tanulmaacuteny
ischaemiaacutes sziacutevizomban keringeacuteseacuteben
redistribucio alakul ki nyugalomban
eacutes gyoacutegyszer indukaacutelt stresszben(44)
SCS indikaacutecioacutek IVPerifeacuteriaacutes vasculaacuteris betegseacutegek
bull lassan progrediaacuteloacute perifeacuteriaacutes vasculaacuteris ischaemia -atherosclerosis (Fontaine 3 4 staacutedium )
bull vazospasticus betegseacuteg (pl Raynaud frostbite) gyoacutegyszeresen eacutersebeacuteszeti műteacutettel nem uralhatoacute veacutegtagfaacutejdalom
bull Buerger-koacuter
bull kontraindikaacutelt laacutebszaacuterfekeacutelygt 3 cm gangreacutena
SCS indikaacutecioacutek VCRPS
CRPS tuumlnetei
1 Harden RN et al Pain 199983211-219 6Birklein F et al Pain 19976949-54
2 Galer BS et al J Pain Symptom Manage 200020286-92 7 Schwartzman RJ Kerrigan J
Neurosurgery 19904057-61
3 Birklein F Handwerker HO Pain 2001 941-6 8 Zyluk A J Hand Surg 200126151-154
4 Rommel O et al Pain 19998095-101 9 Wasner G et al Neuro Clin
199816851-68
5 Thimineur M et al Clin J Pain 199814256-67
Sensory Motor dysfunctionIntense pain12 Weakness
Allodynia13 Decreased range of motion3
Hyperesthesia13 Tremor16
Hyperalgesia13 Dystonia7
Sensory deficits4 Myoclonus7
Decreased muscular strength8
Autonomic Dystrophic Swelling1 Increaseddecreased nailhair growth
Colourtemperature changes6 Skin changes (eg palor plantar fibrosis
Sweating abnormalities6 hyperkeratosis and thin glossy
skin9 )
Courtesy of Robert J Schwartzman MD
SCS indikaacutecioacutek VIAbdominaacutelis eacutes visceraacutelis faacutejdalom
szindroacutemaacutek
bull Faacutejdalom etioloacutegiaacuteja vaacuteltozatos
bull Ok gastrointestinaacutelis gastro-urinaacutelis
musculosceletaacutelis idegrendszeri
bull Megfigyeleacutes Th X myelotomia
daganatos pelvicus faacutejdalmat csillapiacutet
Mechanisms of SCS
bull Gate control theory
bull Direct inhibition of spinothalamic neurons
bull Descending modulatory effects
bull Alteration of sympathetic activity
bull Neurochemical modulation
GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Idegsebeacuteszeti faacutejdalomcsillapiacutetaacutesi lehetőseacutegek neuropaacutetiaacutes faacutejdalomban
bull Ablatiacutev
bull Neuromodulaacutecioacute
Ablatiacutev faacutejdalomcsillapiacutetoacute idegsebeacuteszeti beavatkozaacutesok
bull faacutejdalomvezető paacutelyaacutekat aacutetmetszeacutese roncsolaacutesa destruktiacutev (rizotomiaDREZmyelotomiatermocoagulaacutecioacute)
bull szaacutemos esetben hataacutestalan bull hataacutes aacutetmenetibull maradandoacute hiaacutenytuumlnetbull irreverzibilis magasabb morbiditaacutes bull deafferentaacutecioacutes faacutejdalmak kialakulaacutesa
Funkcionaacutelis idegsebeacuteszetdefiniacutecioacute
bull Koacuteros idegrendszeri műkoumldeacutesek (funkcioacutek) műteacuteti uacuteton toumlrteacutenő befolyaacutesolaacutesa (normalizaacutelaacutesa)
Funkcionaacutelis idegsebeacuteszet -alkalmazaacutesi teruumlletek
bull kroacutenikus faacutejdalom
bull mozgaacuteszavarok
bull spasticitaacutes
bull epilepszia
bull psychochirurgia
bull vegetatiacutev zavarok
Neuromodulaacutecioacute
bull centraacutelis-perifeacuteriaacutes-autonom idegrendszer műkoumldeacuteseacutenek teraacutepiaacutes alteraacutecioacuteja
bull implantaacutelt keacuteszuumlleacutek
bull elektromos gyoacutegyszeres
bull non-destruktiacutev
bull reverzibilis
bull betegseacuteget nem gyoacutegyiacutet
bull műkoumldeacutest eacuteletminőseacuteget javiacutet
Neuromodulaacutecioacute tiacutepusai
bull Elektromos (neurostimulaacutecioacute)
bull Keacutemiai (gyoacutegyszerpumpa)
Neuropathic pain
bull International Association for the Study of Pain defines pain caused by a lesion or disease of the somatosensory nervous system
bull suffer more often from insomnia anxiety and depression1
bull analgetic medication insufficient2
bull SCS has undergone constant technical advancement
Why Neuromodulation
bull Testable
bull Completely reversible
bull Non-destructive
bull No limitation to future therapy
Neurostimulaacutecioacute helye
bull perifeacuteriaacutes ideg PNS PNfS DRGS
bull gerincvelő SCS
bull meacutelyagyi DBS
bull motoros agykeacutereg MCS
Neurostimulaacutecioacutes faacutejdalomcsillapiacutetoacute műteacutetek indikaacutecioacutejaacutenak felaacutelliacutetaacutesa
bull faacutejdalom kezeleacuteseacuteben jaacuteratos szakemberek koumlzoumls doumlnteacutese
bull centrumokban (kivizsgaacutelaacutes kezeleacutes szoumlvődmeacutenyek elhaacuteriacutetaacutesa)
bull multidisciplinaacuteris (ideggyoacutegyaacutesz idegsebeacutesz psychiaacuteter psycholoacutegus anaesthesioloacutegus neuroradioloacutegus elektrofizioloacutegus mozgaacutesterapeuta) munkacsoport
Neurostimulaacutecioacute aacuteltalaacutenos kontraindikaacutecioacutek
(kroacutenikus faacutejdalom)
bull psychiaacutetriai koacuterkeacutepek (aktiacutev psychosis suacutelyos depresszioacute hipochondria szomatizaacutecioacutes betegseacutegek)
bull nem egyuumlttműkoumldő beteg
bull alkoholizmus kaacutebiacutetoacuteszer-eacutelvezet
bull suacutelyos kiacuteseacuterő betegseacuteg (coagulopathia immundeficiencia)
bull maacutes implantaacutelt pacemaker (pl sziacutev)
Neurostimulaacutecioacute műteacuteti szoumlvődmeacutenyek
bull korrigaacutelhatoacutek
bull implantaacutetummal (8-10) kapcsolatos
(elektroacuteda elmozdulaacutes seacuteruumlleacutes elektromos műkoumldeacutes zavar)
bull veacuterzeacutesek (1-5)
bull gyulladaacutesok (5-7)
Spinal cord stimulaacutecioacute (SCS)
bull Legneacutepszerűbb leggyakrabban alkalmazott
bull Első SCS daganatos faacutejdalom (Shealey 1967)
History of Spinal Cord StimulationShealy 1969
bull 1967 ndash Long and Wall PNS
bull 1969 ndash Shealy SCS in humans
bull 1975 ndash Dooley perc electrode
bull Mid 1970s ndash self-powered battery
bull 1980s - programmable quad electrode
bull 1980s -1990s ndash Primary cell IPG
bull 2004 ndash Rechargeable IPG
Clinical studies on SCS continue to support the effectiveness of this
therapy The following charts summarize studies of SCS and its
effects on the quality of life of patients
Reduction of Pain
ReferenceNumber of
PatientsFollow Up Results
Kumar17 410 8 years 74 had gt50 relief
North14 19 3 years 47 had gt50 relief
Barolat9 41 1 year50-65 had good to
excellent relief
Van Buyten18 123 3 years68 had good to excellent
relief
Cameron19 747Up to 59 months
(49 years)
62 had gt50 relief or
significantly reduced pain
scores
SCS indikaacutecioacutek INeuropaacutethiaacutes (neurogeacuten) faacutejdalom
bull Perifeacuteriaacutes idegek seacuteruumlleacutese gyoumlkoumlk plexusok (idegrendszeri hiaacutenytuumlnet) seacuteruumlleacutes okai baleseti műteacutet pl lumbaacutelis discectomia (gyoumlk) nőgyoacutegyaacuteszati (inguinalis ideg) teacuterdműteacutetek (infrapatellaacuteris ideg) mastectomia (costo-brachiaacutelis ideg)
bull veacutegtag-amputaacutecioacute csonkfaacutejdalom jobban mint a fantom faacutejdalombull post-herpeses neuralgia amennyiben a bőreacuterzeacutes reacuteszlegesen megtartottbull post-irradiaacutecioacutes plexopaacutetiabull polyneuropaacutetiaacutek (diabeteses alkoholos) post-kemoteraacutepiaacutes (amennyiben a vastag rostok
műkoumldeacutese reacuteszlegesen megtartott)bull gerincvelő incomplett seacuteruumlleacutese -amennyiben a vastag eacuterzőrostok műkoumldeacutese megtartott eacutes a
segmentaacutelis faacutejdalom a seacuteruumlleacutes magassaacutegaacuteban leacutep felbull cervicaacutelis eacutes lumbosacralis radiculopaacutetiaacutek (compresszioacute ischaemia sebeacuteszi baleset
arachnoiditisbull CRPS II (causalga)bull DE bull plexus avulsioacute syringomyelia faacutejdalom nem csillapiacutethatoacutek bull nincs egyeteacuterteacutes a CRPS I (reflex sympaticus dystrophia)
SCS indikaacutecioacutek II
bull Kevert faacutejdalom szindroacutemaacutek
Falied back surgery syndroma = FBSS koraacutebbi gerincsebeacuteszeti beavatkozaacutes (postoperatiacutev fibrosis arachnoiditis)
Posztlaminektomiaacutes szindroacutemaangolszaacutesz failed back surgery szindroacutemaacutenak (FBSS)
bull faacutejdalom lokalizaacutecioacute alsoacute aacutegyeacuteki gerinc far
alsoacute veacutegtagok
bull etioloacutegia arachnoiditis epiduraacutelis heg
radiculitis mikro-instabilitaacutes rec
porckorongseacuterv gyulladaacutes
bull tapasztalatok alsoacute veacutegtagba terjedő
faacutejdalomra SCS hateacutekony
bull axiaacutelis faacutejdalmakra nem bizonyiacutetott
Incidencia FBSS
bull ranges 5 - 50
bull postdiscectomy 10-40
Etiologia FBSS
bull Scar tissue that forms around the surgery site interrupting normal neurological functioning
bull technicalities of the operation are not successful the performing surgeon had poor technique andor there is iatrogenic injury present
bull surgery is not performed at the site that causes the pain
bull surgery performed is not actually necessarybull patient is a poor fit for a successful surgerybull diagnosis was incorrectbull Complications of surgery arise
1 Anderson VC et al Current review of pain 20004105-11 5 Vaccaro AR et al Spine 200126 (24) S111-82 Leveque JC et al Neuromodulation 200141-9 6 Spengler DM et al Spine 19805356-603 Dario A et al Neuromodulation 20014105-110 7 Fager CA Freidberg SR Spine 1980587-944 Ohnmeiss DD et al The Spine Journal 2001358-363 8 Long DM Surgical management of pain 2002 354-64
FBSS okai eacutes tuumlnetei
bull FBSS cause1-7
ndash irreversible nerve injury
ndash surgical complications
ndash psychosocial problems
ndash inappropriate selection of patients for surgery
ndash recurrent herniation
ndash wrong level of operation
bull FBSS symptoms348
ndash lumbosacral postoperative fibrosis andor arachnoiditis
ndash root lesion
ndash dorsal compartment syndrome
ndash lateral spinal stenosis
SCS indikaacutecioacutek IIIAngina pectoris
bull New York Heart Association III-IV csoport (szignifikaacutens coronaacuteria stenosis egy vagy toumlbb szűkuumllet 70 )
bull myocardiaacutelis ischaemia reverzibilis angina gyoacutegyszeres revascularizaacutecioacutes beavatkozaacutesokkal nem enyhiacutethető
bull eacuteletminőseacuteguarr nitro-glicerin felhasznaacutelaacutesdarr anginaacutes rohamok szaacutemadarr jaacuteraacutestaacutevolsaacuteguarr
bull SCS anti-ischaemiaacutes hataacutes
bull nincs bizonyiacuteteacutek SCS hateacutekonysaacutegra instabil angina acut myocardiaacutelis infarctus vazospasticus angia maacutes sziacutevbetegseacuteg okozta anginaacutes faacutejdalmak csillapiacutetaacutesaacutera
Anginaacutes faacutejdalom
SCS tanulmaacutenyok hateacutekonysaacuteg I
bull Nienke (45 ) PT 1 eacutev koumlveteacutes eacuteletminőseacuteg szociaacutelis mentaacutelis fizikaacutelis teljesiacutetmeacuteny szignifikaacutensan javul
bull Hautvast (46) stabil angina pectorisban RT 6 heacutet koumlveteacutes
Randomizaacutelaacutes a stimulaacutetor OFF b csoport 3x1 oacuteranap ON vagy hirtelen anginaacuteban
anginaacutes rohamszaacutem csoumlkken
fizikai teljesiacutetőkeacutepesseacuteg javul
sublinguaacutelis nitraacutet felhasznaacutelaacutes csoumlkken
EKG-n az ischaemiaacutes epizoacutedusok csoumlkkennek
ST depresszioacute enyhuumll eacuteletminőseacuteg javul
anginaacutes faacutejdalom csoumlkken
SCS indikaacutecioacutek IIIAngina pectoris
bull tanulmaacutenyok eredmeacutenyei kedvezőek (39-43)
bull teraacutepiaacutes hataacutes hosszuacute taacutevuacute
bull nitraacutet bevitel csoumlkkenthető
bull faacutejdalomcsillapiacutetoacute hataacutesuacute
bull sziacutevizom veacuterkeringeacutes javul
bull PET tanulmaacuteny
ischaemiaacutes sziacutevizomban keringeacuteseacuteben
redistribucio alakul ki nyugalomban
eacutes gyoacutegyszer indukaacutelt stresszben(44)
SCS indikaacutecioacutek IVPerifeacuteriaacutes vasculaacuteris betegseacutegek
bull lassan progrediaacuteloacute perifeacuteriaacutes vasculaacuteris ischaemia -atherosclerosis (Fontaine 3 4 staacutedium )
bull vazospasticus betegseacuteg (pl Raynaud frostbite) gyoacutegyszeresen eacutersebeacuteszeti műteacutettel nem uralhatoacute veacutegtagfaacutejdalom
bull Buerger-koacuter
bull kontraindikaacutelt laacutebszaacuterfekeacutelygt 3 cm gangreacutena
SCS indikaacutecioacutek VCRPS
CRPS tuumlnetei
1 Harden RN et al Pain 199983211-219 6Birklein F et al Pain 19976949-54
2 Galer BS et al J Pain Symptom Manage 200020286-92 7 Schwartzman RJ Kerrigan J
Neurosurgery 19904057-61
3 Birklein F Handwerker HO Pain 2001 941-6 8 Zyluk A J Hand Surg 200126151-154
4 Rommel O et al Pain 19998095-101 9 Wasner G et al Neuro Clin
199816851-68
5 Thimineur M et al Clin J Pain 199814256-67
Sensory Motor dysfunctionIntense pain12 Weakness
Allodynia13 Decreased range of motion3
Hyperesthesia13 Tremor16
Hyperalgesia13 Dystonia7
Sensory deficits4 Myoclonus7
Decreased muscular strength8
Autonomic Dystrophic Swelling1 Increaseddecreased nailhair growth
Colourtemperature changes6 Skin changes (eg palor plantar fibrosis
Sweating abnormalities6 hyperkeratosis and thin glossy
skin9 )
Courtesy of Robert J Schwartzman MD
SCS indikaacutecioacutek VIAbdominaacutelis eacutes visceraacutelis faacutejdalom
szindroacutemaacutek
bull Faacutejdalom etioloacutegiaacuteja vaacuteltozatos
bull Ok gastrointestinaacutelis gastro-urinaacutelis
musculosceletaacutelis idegrendszeri
bull Megfigyeleacutes Th X myelotomia
daganatos pelvicus faacutejdalmat csillapiacutet
Mechanisms of SCS
bull Gate control theory
bull Direct inhibition of spinothalamic neurons
bull Descending modulatory effects
bull Alteration of sympathetic activity
bull Neurochemical modulation
GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Ablatiacutev faacutejdalomcsillapiacutetoacute idegsebeacuteszeti beavatkozaacutesok
bull faacutejdalomvezető paacutelyaacutekat aacutetmetszeacutese roncsolaacutesa destruktiacutev (rizotomiaDREZmyelotomiatermocoagulaacutecioacute)
bull szaacutemos esetben hataacutestalan bull hataacutes aacutetmenetibull maradandoacute hiaacutenytuumlnetbull irreverzibilis magasabb morbiditaacutes bull deafferentaacutecioacutes faacutejdalmak kialakulaacutesa
Funkcionaacutelis idegsebeacuteszetdefiniacutecioacute
bull Koacuteros idegrendszeri műkoumldeacutesek (funkcioacutek) műteacuteti uacuteton toumlrteacutenő befolyaacutesolaacutesa (normalizaacutelaacutesa)
Funkcionaacutelis idegsebeacuteszet -alkalmazaacutesi teruumlletek
bull kroacutenikus faacutejdalom
bull mozgaacuteszavarok
bull spasticitaacutes
bull epilepszia
bull psychochirurgia
bull vegetatiacutev zavarok
Neuromodulaacutecioacute
bull centraacutelis-perifeacuteriaacutes-autonom idegrendszer műkoumldeacuteseacutenek teraacutepiaacutes alteraacutecioacuteja
bull implantaacutelt keacuteszuumlleacutek
bull elektromos gyoacutegyszeres
bull non-destruktiacutev
bull reverzibilis
bull betegseacuteget nem gyoacutegyiacutet
bull műkoumldeacutest eacuteletminőseacuteget javiacutet
Neuromodulaacutecioacute tiacutepusai
bull Elektromos (neurostimulaacutecioacute)
bull Keacutemiai (gyoacutegyszerpumpa)
Neuropathic pain
bull International Association for the Study of Pain defines pain caused by a lesion or disease of the somatosensory nervous system
bull suffer more often from insomnia anxiety and depression1
bull analgetic medication insufficient2
bull SCS has undergone constant technical advancement
Why Neuromodulation
bull Testable
bull Completely reversible
bull Non-destructive
bull No limitation to future therapy
Neurostimulaacutecioacute helye
bull perifeacuteriaacutes ideg PNS PNfS DRGS
bull gerincvelő SCS
bull meacutelyagyi DBS
bull motoros agykeacutereg MCS
Neurostimulaacutecioacutes faacutejdalomcsillapiacutetoacute műteacutetek indikaacutecioacutejaacutenak felaacutelliacutetaacutesa
bull faacutejdalom kezeleacuteseacuteben jaacuteratos szakemberek koumlzoumls doumlnteacutese
bull centrumokban (kivizsgaacutelaacutes kezeleacutes szoumlvődmeacutenyek elhaacuteriacutetaacutesa)
bull multidisciplinaacuteris (ideggyoacutegyaacutesz idegsebeacutesz psychiaacuteter psycholoacutegus anaesthesioloacutegus neuroradioloacutegus elektrofizioloacutegus mozgaacutesterapeuta) munkacsoport
Neurostimulaacutecioacute aacuteltalaacutenos kontraindikaacutecioacutek
(kroacutenikus faacutejdalom)
bull psychiaacutetriai koacuterkeacutepek (aktiacutev psychosis suacutelyos depresszioacute hipochondria szomatizaacutecioacutes betegseacutegek)
bull nem egyuumlttműkoumldő beteg
bull alkoholizmus kaacutebiacutetoacuteszer-eacutelvezet
bull suacutelyos kiacuteseacuterő betegseacuteg (coagulopathia immundeficiencia)
bull maacutes implantaacutelt pacemaker (pl sziacutev)
Neurostimulaacutecioacute műteacuteti szoumlvődmeacutenyek
bull korrigaacutelhatoacutek
bull implantaacutetummal (8-10) kapcsolatos
(elektroacuteda elmozdulaacutes seacuteruumlleacutes elektromos műkoumldeacutes zavar)
bull veacuterzeacutesek (1-5)
bull gyulladaacutesok (5-7)
Spinal cord stimulaacutecioacute (SCS)
bull Legneacutepszerűbb leggyakrabban alkalmazott
bull Első SCS daganatos faacutejdalom (Shealey 1967)
History of Spinal Cord StimulationShealy 1969
bull 1967 ndash Long and Wall PNS
bull 1969 ndash Shealy SCS in humans
bull 1975 ndash Dooley perc electrode
bull Mid 1970s ndash self-powered battery
bull 1980s - programmable quad electrode
bull 1980s -1990s ndash Primary cell IPG
bull 2004 ndash Rechargeable IPG
Clinical studies on SCS continue to support the effectiveness of this
therapy The following charts summarize studies of SCS and its
effects on the quality of life of patients
Reduction of Pain
ReferenceNumber of
PatientsFollow Up Results
Kumar17 410 8 years 74 had gt50 relief
North14 19 3 years 47 had gt50 relief
Barolat9 41 1 year50-65 had good to
excellent relief
Van Buyten18 123 3 years68 had good to excellent
relief
Cameron19 747Up to 59 months
(49 years)
62 had gt50 relief or
significantly reduced pain
scores
SCS indikaacutecioacutek INeuropaacutethiaacutes (neurogeacuten) faacutejdalom
bull Perifeacuteriaacutes idegek seacuteruumlleacutese gyoumlkoumlk plexusok (idegrendszeri hiaacutenytuumlnet) seacuteruumlleacutes okai baleseti műteacutet pl lumbaacutelis discectomia (gyoumlk) nőgyoacutegyaacuteszati (inguinalis ideg) teacuterdműteacutetek (infrapatellaacuteris ideg) mastectomia (costo-brachiaacutelis ideg)
bull veacutegtag-amputaacutecioacute csonkfaacutejdalom jobban mint a fantom faacutejdalombull post-herpeses neuralgia amennyiben a bőreacuterzeacutes reacuteszlegesen megtartottbull post-irradiaacutecioacutes plexopaacutetiabull polyneuropaacutetiaacutek (diabeteses alkoholos) post-kemoteraacutepiaacutes (amennyiben a vastag rostok
műkoumldeacutese reacuteszlegesen megtartott)bull gerincvelő incomplett seacuteruumlleacutese -amennyiben a vastag eacuterzőrostok műkoumldeacutese megtartott eacutes a
segmentaacutelis faacutejdalom a seacuteruumlleacutes magassaacutegaacuteban leacutep felbull cervicaacutelis eacutes lumbosacralis radiculopaacutetiaacutek (compresszioacute ischaemia sebeacuteszi baleset
arachnoiditisbull CRPS II (causalga)bull DE bull plexus avulsioacute syringomyelia faacutejdalom nem csillapiacutethatoacutek bull nincs egyeteacuterteacutes a CRPS I (reflex sympaticus dystrophia)
SCS indikaacutecioacutek II
bull Kevert faacutejdalom szindroacutemaacutek
Falied back surgery syndroma = FBSS koraacutebbi gerincsebeacuteszeti beavatkozaacutes (postoperatiacutev fibrosis arachnoiditis)
Posztlaminektomiaacutes szindroacutemaangolszaacutesz failed back surgery szindroacutemaacutenak (FBSS)
bull faacutejdalom lokalizaacutecioacute alsoacute aacutegyeacuteki gerinc far
alsoacute veacutegtagok
bull etioloacutegia arachnoiditis epiduraacutelis heg
radiculitis mikro-instabilitaacutes rec
porckorongseacuterv gyulladaacutes
bull tapasztalatok alsoacute veacutegtagba terjedő
faacutejdalomra SCS hateacutekony
bull axiaacutelis faacutejdalmakra nem bizonyiacutetott
Incidencia FBSS
bull ranges 5 - 50
bull postdiscectomy 10-40
Etiologia FBSS
bull Scar tissue that forms around the surgery site interrupting normal neurological functioning
bull technicalities of the operation are not successful the performing surgeon had poor technique andor there is iatrogenic injury present
bull surgery is not performed at the site that causes the pain
bull surgery performed is not actually necessarybull patient is a poor fit for a successful surgerybull diagnosis was incorrectbull Complications of surgery arise
1 Anderson VC et al Current review of pain 20004105-11 5 Vaccaro AR et al Spine 200126 (24) S111-82 Leveque JC et al Neuromodulation 200141-9 6 Spengler DM et al Spine 19805356-603 Dario A et al Neuromodulation 20014105-110 7 Fager CA Freidberg SR Spine 1980587-944 Ohnmeiss DD et al The Spine Journal 2001358-363 8 Long DM Surgical management of pain 2002 354-64
FBSS okai eacutes tuumlnetei
bull FBSS cause1-7
ndash irreversible nerve injury
ndash surgical complications
ndash psychosocial problems
ndash inappropriate selection of patients for surgery
ndash recurrent herniation
ndash wrong level of operation
bull FBSS symptoms348
ndash lumbosacral postoperative fibrosis andor arachnoiditis
ndash root lesion
ndash dorsal compartment syndrome
ndash lateral spinal stenosis
SCS indikaacutecioacutek IIIAngina pectoris
bull New York Heart Association III-IV csoport (szignifikaacutens coronaacuteria stenosis egy vagy toumlbb szűkuumllet 70 )
bull myocardiaacutelis ischaemia reverzibilis angina gyoacutegyszeres revascularizaacutecioacutes beavatkozaacutesokkal nem enyhiacutethető
bull eacuteletminőseacuteguarr nitro-glicerin felhasznaacutelaacutesdarr anginaacutes rohamok szaacutemadarr jaacuteraacutestaacutevolsaacuteguarr
bull SCS anti-ischaemiaacutes hataacutes
bull nincs bizonyiacuteteacutek SCS hateacutekonysaacutegra instabil angina acut myocardiaacutelis infarctus vazospasticus angia maacutes sziacutevbetegseacuteg okozta anginaacutes faacutejdalmak csillapiacutetaacutesaacutera
Anginaacutes faacutejdalom
SCS tanulmaacutenyok hateacutekonysaacuteg I
bull Nienke (45 ) PT 1 eacutev koumlveteacutes eacuteletminőseacuteg szociaacutelis mentaacutelis fizikaacutelis teljesiacutetmeacuteny szignifikaacutensan javul
bull Hautvast (46) stabil angina pectorisban RT 6 heacutet koumlveteacutes
Randomizaacutelaacutes a stimulaacutetor OFF b csoport 3x1 oacuteranap ON vagy hirtelen anginaacuteban
anginaacutes rohamszaacutem csoumlkken
fizikai teljesiacutetőkeacutepesseacuteg javul
sublinguaacutelis nitraacutet felhasznaacutelaacutes csoumlkken
EKG-n az ischaemiaacutes epizoacutedusok csoumlkkennek
ST depresszioacute enyhuumll eacuteletminőseacuteg javul
anginaacutes faacutejdalom csoumlkken
SCS indikaacutecioacutek IIIAngina pectoris
bull tanulmaacutenyok eredmeacutenyei kedvezőek (39-43)
bull teraacutepiaacutes hataacutes hosszuacute taacutevuacute
bull nitraacutet bevitel csoumlkkenthető
bull faacutejdalomcsillapiacutetoacute hataacutesuacute
bull sziacutevizom veacuterkeringeacutes javul
bull PET tanulmaacuteny
ischaemiaacutes sziacutevizomban keringeacuteseacuteben
redistribucio alakul ki nyugalomban
eacutes gyoacutegyszer indukaacutelt stresszben(44)
SCS indikaacutecioacutek IVPerifeacuteriaacutes vasculaacuteris betegseacutegek
bull lassan progrediaacuteloacute perifeacuteriaacutes vasculaacuteris ischaemia -atherosclerosis (Fontaine 3 4 staacutedium )
bull vazospasticus betegseacuteg (pl Raynaud frostbite) gyoacutegyszeresen eacutersebeacuteszeti műteacutettel nem uralhatoacute veacutegtagfaacutejdalom
bull Buerger-koacuter
bull kontraindikaacutelt laacutebszaacuterfekeacutelygt 3 cm gangreacutena
SCS indikaacutecioacutek VCRPS
CRPS tuumlnetei
1 Harden RN et al Pain 199983211-219 6Birklein F et al Pain 19976949-54
2 Galer BS et al J Pain Symptom Manage 200020286-92 7 Schwartzman RJ Kerrigan J
Neurosurgery 19904057-61
3 Birklein F Handwerker HO Pain 2001 941-6 8 Zyluk A J Hand Surg 200126151-154
4 Rommel O et al Pain 19998095-101 9 Wasner G et al Neuro Clin
199816851-68
5 Thimineur M et al Clin J Pain 199814256-67
Sensory Motor dysfunctionIntense pain12 Weakness
Allodynia13 Decreased range of motion3
Hyperesthesia13 Tremor16
Hyperalgesia13 Dystonia7
Sensory deficits4 Myoclonus7
Decreased muscular strength8
Autonomic Dystrophic Swelling1 Increaseddecreased nailhair growth
Colourtemperature changes6 Skin changes (eg palor plantar fibrosis
Sweating abnormalities6 hyperkeratosis and thin glossy
skin9 )
Courtesy of Robert J Schwartzman MD
SCS indikaacutecioacutek VIAbdominaacutelis eacutes visceraacutelis faacutejdalom
szindroacutemaacutek
bull Faacutejdalom etioloacutegiaacuteja vaacuteltozatos
bull Ok gastrointestinaacutelis gastro-urinaacutelis
musculosceletaacutelis idegrendszeri
bull Megfigyeleacutes Th X myelotomia
daganatos pelvicus faacutejdalmat csillapiacutet
Mechanisms of SCS
bull Gate control theory
bull Direct inhibition of spinothalamic neurons
bull Descending modulatory effects
bull Alteration of sympathetic activity
bull Neurochemical modulation
GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Funkcionaacutelis idegsebeacuteszetdefiniacutecioacute
bull Koacuteros idegrendszeri műkoumldeacutesek (funkcioacutek) műteacuteti uacuteton toumlrteacutenő befolyaacutesolaacutesa (normalizaacutelaacutesa)
Funkcionaacutelis idegsebeacuteszet -alkalmazaacutesi teruumlletek
bull kroacutenikus faacutejdalom
bull mozgaacuteszavarok
bull spasticitaacutes
bull epilepszia
bull psychochirurgia
bull vegetatiacutev zavarok
Neuromodulaacutecioacute
bull centraacutelis-perifeacuteriaacutes-autonom idegrendszer műkoumldeacuteseacutenek teraacutepiaacutes alteraacutecioacuteja
bull implantaacutelt keacuteszuumlleacutek
bull elektromos gyoacutegyszeres
bull non-destruktiacutev
bull reverzibilis
bull betegseacuteget nem gyoacutegyiacutet
bull műkoumldeacutest eacuteletminőseacuteget javiacutet
Neuromodulaacutecioacute tiacutepusai
bull Elektromos (neurostimulaacutecioacute)
bull Keacutemiai (gyoacutegyszerpumpa)
Neuropathic pain
bull International Association for the Study of Pain defines pain caused by a lesion or disease of the somatosensory nervous system
bull suffer more often from insomnia anxiety and depression1
bull analgetic medication insufficient2
bull SCS has undergone constant technical advancement
Why Neuromodulation
bull Testable
bull Completely reversible
bull Non-destructive
bull No limitation to future therapy
Neurostimulaacutecioacute helye
bull perifeacuteriaacutes ideg PNS PNfS DRGS
bull gerincvelő SCS
bull meacutelyagyi DBS
bull motoros agykeacutereg MCS
Neurostimulaacutecioacutes faacutejdalomcsillapiacutetoacute műteacutetek indikaacutecioacutejaacutenak felaacutelliacutetaacutesa
bull faacutejdalom kezeleacuteseacuteben jaacuteratos szakemberek koumlzoumls doumlnteacutese
bull centrumokban (kivizsgaacutelaacutes kezeleacutes szoumlvődmeacutenyek elhaacuteriacutetaacutesa)
bull multidisciplinaacuteris (ideggyoacutegyaacutesz idegsebeacutesz psychiaacuteter psycholoacutegus anaesthesioloacutegus neuroradioloacutegus elektrofizioloacutegus mozgaacutesterapeuta) munkacsoport
Neurostimulaacutecioacute aacuteltalaacutenos kontraindikaacutecioacutek
(kroacutenikus faacutejdalom)
bull psychiaacutetriai koacuterkeacutepek (aktiacutev psychosis suacutelyos depresszioacute hipochondria szomatizaacutecioacutes betegseacutegek)
bull nem egyuumlttműkoumldő beteg
bull alkoholizmus kaacutebiacutetoacuteszer-eacutelvezet
bull suacutelyos kiacuteseacuterő betegseacuteg (coagulopathia immundeficiencia)
bull maacutes implantaacutelt pacemaker (pl sziacutev)
Neurostimulaacutecioacute műteacuteti szoumlvődmeacutenyek
bull korrigaacutelhatoacutek
bull implantaacutetummal (8-10) kapcsolatos
(elektroacuteda elmozdulaacutes seacuteruumlleacutes elektromos műkoumldeacutes zavar)
bull veacuterzeacutesek (1-5)
bull gyulladaacutesok (5-7)
Spinal cord stimulaacutecioacute (SCS)
bull Legneacutepszerűbb leggyakrabban alkalmazott
bull Első SCS daganatos faacutejdalom (Shealey 1967)
History of Spinal Cord StimulationShealy 1969
bull 1967 ndash Long and Wall PNS
bull 1969 ndash Shealy SCS in humans
bull 1975 ndash Dooley perc electrode
bull Mid 1970s ndash self-powered battery
bull 1980s - programmable quad electrode
bull 1980s -1990s ndash Primary cell IPG
bull 2004 ndash Rechargeable IPG
Clinical studies on SCS continue to support the effectiveness of this
therapy The following charts summarize studies of SCS and its
effects on the quality of life of patients
Reduction of Pain
ReferenceNumber of
PatientsFollow Up Results
Kumar17 410 8 years 74 had gt50 relief
North14 19 3 years 47 had gt50 relief
Barolat9 41 1 year50-65 had good to
excellent relief
Van Buyten18 123 3 years68 had good to excellent
relief
Cameron19 747Up to 59 months
(49 years)
62 had gt50 relief or
significantly reduced pain
scores
SCS indikaacutecioacutek INeuropaacutethiaacutes (neurogeacuten) faacutejdalom
bull Perifeacuteriaacutes idegek seacuteruumlleacutese gyoumlkoumlk plexusok (idegrendszeri hiaacutenytuumlnet) seacuteruumlleacutes okai baleseti műteacutet pl lumbaacutelis discectomia (gyoumlk) nőgyoacutegyaacuteszati (inguinalis ideg) teacuterdműteacutetek (infrapatellaacuteris ideg) mastectomia (costo-brachiaacutelis ideg)
bull veacutegtag-amputaacutecioacute csonkfaacutejdalom jobban mint a fantom faacutejdalombull post-herpeses neuralgia amennyiben a bőreacuterzeacutes reacuteszlegesen megtartottbull post-irradiaacutecioacutes plexopaacutetiabull polyneuropaacutetiaacutek (diabeteses alkoholos) post-kemoteraacutepiaacutes (amennyiben a vastag rostok
műkoumldeacutese reacuteszlegesen megtartott)bull gerincvelő incomplett seacuteruumlleacutese -amennyiben a vastag eacuterzőrostok műkoumldeacutese megtartott eacutes a
segmentaacutelis faacutejdalom a seacuteruumlleacutes magassaacutegaacuteban leacutep felbull cervicaacutelis eacutes lumbosacralis radiculopaacutetiaacutek (compresszioacute ischaemia sebeacuteszi baleset
arachnoiditisbull CRPS II (causalga)bull DE bull plexus avulsioacute syringomyelia faacutejdalom nem csillapiacutethatoacutek bull nincs egyeteacuterteacutes a CRPS I (reflex sympaticus dystrophia)
SCS indikaacutecioacutek II
bull Kevert faacutejdalom szindroacutemaacutek
Falied back surgery syndroma = FBSS koraacutebbi gerincsebeacuteszeti beavatkozaacutes (postoperatiacutev fibrosis arachnoiditis)
Posztlaminektomiaacutes szindroacutemaangolszaacutesz failed back surgery szindroacutemaacutenak (FBSS)
bull faacutejdalom lokalizaacutecioacute alsoacute aacutegyeacuteki gerinc far
alsoacute veacutegtagok
bull etioloacutegia arachnoiditis epiduraacutelis heg
radiculitis mikro-instabilitaacutes rec
porckorongseacuterv gyulladaacutes
bull tapasztalatok alsoacute veacutegtagba terjedő
faacutejdalomra SCS hateacutekony
bull axiaacutelis faacutejdalmakra nem bizonyiacutetott
Incidencia FBSS
bull ranges 5 - 50
bull postdiscectomy 10-40
Etiologia FBSS
bull Scar tissue that forms around the surgery site interrupting normal neurological functioning
bull technicalities of the operation are not successful the performing surgeon had poor technique andor there is iatrogenic injury present
bull surgery is not performed at the site that causes the pain
bull surgery performed is not actually necessarybull patient is a poor fit for a successful surgerybull diagnosis was incorrectbull Complications of surgery arise
1 Anderson VC et al Current review of pain 20004105-11 5 Vaccaro AR et al Spine 200126 (24) S111-82 Leveque JC et al Neuromodulation 200141-9 6 Spengler DM et al Spine 19805356-603 Dario A et al Neuromodulation 20014105-110 7 Fager CA Freidberg SR Spine 1980587-944 Ohnmeiss DD et al The Spine Journal 2001358-363 8 Long DM Surgical management of pain 2002 354-64
FBSS okai eacutes tuumlnetei
bull FBSS cause1-7
ndash irreversible nerve injury
ndash surgical complications
ndash psychosocial problems
ndash inappropriate selection of patients for surgery
ndash recurrent herniation
ndash wrong level of operation
bull FBSS symptoms348
ndash lumbosacral postoperative fibrosis andor arachnoiditis
ndash root lesion
ndash dorsal compartment syndrome
ndash lateral spinal stenosis
SCS indikaacutecioacutek IIIAngina pectoris
bull New York Heart Association III-IV csoport (szignifikaacutens coronaacuteria stenosis egy vagy toumlbb szűkuumllet 70 )
bull myocardiaacutelis ischaemia reverzibilis angina gyoacutegyszeres revascularizaacutecioacutes beavatkozaacutesokkal nem enyhiacutethető
bull eacuteletminőseacuteguarr nitro-glicerin felhasznaacutelaacutesdarr anginaacutes rohamok szaacutemadarr jaacuteraacutestaacutevolsaacuteguarr
bull SCS anti-ischaemiaacutes hataacutes
bull nincs bizonyiacuteteacutek SCS hateacutekonysaacutegra instabil angina acut myocardiaacutelis infarctus vazospasticus angia maacutes sziacutevbetegseacuteg okozta anginaacutes faacutejdalmak csillapiacutetaacutesaacutera
Anginaacutes faacutejdalom
SCS tanulmaacutenyok hateacutekonysaacuteg I
bull Nienke (45 ) PT 1 eacutev koumlveteacutes eacuteletminőseacuteg szociaacutelis mentaacutelis fizikaacutelis teljesiacutetmeacuteny szignifikaacutensan javul
bull Hautvast (46) stabil angina pectorisban RT 6 heacutet koumlveteacutes
Randomizaacutelaacutes a stimulaacutetor OFF b csoport 3x1 oacuteranap ON vagy hirtelen anginaacuteban
anginaacutes rohamszaacutem csoumlkken
fizikai teljesiacutetőkeacutepesseacuteg javul
sublinguaacutelis nitraacutet felhasznaacutelaacutes csoumlkken
EKG-n az ischaemiaacutes epizoacutedusok csoumlkkennek
ST depresszioacute enyhuumll eacuteletminőseacuteg javul
anginaacutes faacutejdalom csoumlkken
SCS indikaacutecioacutek IIIAngina pectoris
bull tanulmaacutenyok eredmeacutenyei kedvezőek (39-43)
bull teraacutepiaacutes hataacutes hosszuacute taacutevuacute
bull nitraacutet bevitel csoumlkkenthető
bull faacutejdalomcsillapiacutetoacute hataacutesuacute
bull sziacutevizom veacuterkeringeacutes javul
bull PET tanulmaacuteny
ischaemiaacutes sziacutevizomban keringeacuteseacuteben
redistribucio alakul ki nyugalomban
eacutes gyoacutegyszer indukaacutelt stresszben(44)
SCS indikaacutecioacutek IVPerifeacuteriaacutes vasculaacuteris betegseacutegek
bull lassan progrediaacuteloacute perifeacuteriaacutes vasculaacuteris ischaemia -atherosclerosis (Fontaine 3 4 staacutedium )
bull vazospasticus betegseacuteg (pl Raynaud frostbite) gyoacutegyszeresen eacutersebeacuteszeti műteacutettel nem uralhatoacute veacutegtagfaacutejdalom
bull Buerger-koacuter
bull kontraindikaacutelt laacutebszaacuterfekeacutelygt 3 cm gangreacutena
SCS indikaacutecioacutek VCRPS
CRPS tuumlnetei
1 Harden RN et al Pain 199983211-219 6Birklein F et al Pain 19976949-54
2 Galer BS et al J Pain Symptom Manage 200020286-92 7 Schwartzman RJ Kerrigan J
Neurosurgery 19904057-61
3 Birklein F Handwerker HO Pain 2001 941-6 8 Zyluk A J Hand Surg 200126151-154
4 Rommel O et al Pain 19998095-101 9 Wasner G et al Neuro Clin
199816851-68
5 Thimineur M et al Clin J Pain 199814256-67
Sensory Motor dysfunctionIntense pain12 Weakness
Allodynia13 Decreased range of motion3
Hyperesthesia13 Tremor16
Hyperalgesia13 Dystonia7
Sensory deficits4 Myoclonus7
Decreased muscular strength8
Autonomic Dystrophic Swelling1 Increaseddecreased nailhair growth
Colourtemperature changes6 Skin changes (eg palor plantar fibrosis
Sweating abnormalities6 hyperkeratosis and thin glossy
skin9 )
Courtesy of Robert J Schwartzman MD
SCS indikaacutecioacutek VIAbdominaacutelis eacutes visceraacutelis faacutejdalom
szindroacutemaacutek
bull Faacutejdalom etioloacutegiaacuteja vaacuteltozatos
bull Ok gastrointestinaacutelis gastro-urinaacutelis
musculosceletaacutelis idegrendszeri
bull Megfigyeleacutes Th X myelotomia
daganatos pelvicus faacutejdalmat csillapiacutet
Mechanisms of SCS
bull Gate control theory
bull Direct inhibition of spinothalamic neurons
bull Descending modulatory effects
bull Alteration of sympathetic activity
bull Neurochemical modulation
GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Funkcionaacutelis idegsebeacuteszet -alkalmazaacutesi teruumlletek
bull kroacutenikus faacutejdalom
bull mozgaacuteszavarok
bull spasticitaacutes
bull epilepszia
bull psychochirurgia
bull vegetatiacutev zavarok
Neuromodulaacutecioacute
bull centraacutelis-perifeacuteriaacutes-autonom idegrendszer műkoumldeacuteseacutenek teraacutepiaacutes alteraacutecioacuteja
bull implantaacutelt keacuteszuumlleacutek
bull elektromos gyoacutegyszeres
bull non-destruktiacutev
bull reverzibilis
bull betegseacuteget nem gyoacutegyiacutet
bull műkoumldeacutest eacuteletminőseacuteget javiacutet
Neuromodulaacutecioacute tiacutepusai
bull Elektromos (neurostimulaacutecioacute)
bull Keacutemiai (gyoacutegyszerpumpa)
Neuropathic pain
bull International Association for the Study of Pain defines pain caused by a lesion or disease of the somatosensory nervous system
bull suffer more often from insomnia anxiety and depression1
bull analgetic medication insufficient2
bull SCS has undergone constant technical advancement
Why Neuromodulation
bull Testable
bull Completely reversible
bull Non-destructive
bull No limitation to future therapy
Neurostimulaacutecioacute helye
bull perifeacuteriaacutes ideg PNS PNfS DRGS
bull gerincvelő SCS
bull meacutelyagyi DBS
bull motoros agykeacutereg MCS
Neurostimulaacutecioacutes faacutejdalomcsillapiacutetoacute műteacutetek indikaacutecioacutejaacutenak felaacutelliacutetaacutesa
bull faacutejdalom kezeleacuteseacuteben jaacuteratos szakemberek koumlzoumls doumlnteacutese
bull centrumokban (kivizsgaacutelaacutes kezeleacutes szoumlvődmeacutenyek elhaacuteriacutetaacutesa)
bull multidisciplinaacuteris (ideggyoacutegyaacutesz idegsebeacutesz psychiaacuteter psycholoacutegus anaesthesioloacutegus neuroradioloacutegus elektrofizioloacutegus mozgaacutesterapeuta) munkacsoport
Neurostimulaacutecioacute aacuteltalaacutenos kontraindikaacutecioacutek
(kroacutenikus faacutejdalom)
bull psychiaacutetriai koacuterkeacutepek (aktiacutev psychosis suacutelyos depresszioacute hipochondria szomatizaacutecioacutes betegseacutegek)
bull nem egyuumlttműkoumldő beteg
bull alkoholizmus kaacutebiacutetoacuteszer-eacutelvezet
bull suacutelyos kiacuteseacuterő betegseacuteg (coagulopathia immundeficiencia)
bull maacutes implantaacutelt pacemaker (pl sziacutev)
Neurostimulaacutecioacute műteacuteti szoumlvődmeacutenyek
bull korrigaacutelhatoacutek
bull implantaacutetummal (8-10) kapcsolatos
(elektroacuteda elmozdulaacutes seacuteruumlleacutes elektromos műkoumldeacutes zavar)
bull veacuterzeacutesek (1-5)
bull gyulladaacutesok (5-7)
Spinal cord stimulaacutecioacute (SCS)
bull Legneacutepszerűbb leggyakrabban alkalmazott
bull Első SCS daganatos faacutejdalom (Shealey 1967)
History of Spinal Cord StimulationShealy 1969
bull 1967 ndash Long and Wall PNS
bull 1969 ndash Shealy SCS in humans
bull 1975 ndash Dooley perc electrode
bull Mid 1970s ndash self-powered battery
bull 1980s - programmable quad electrode
bull 1980s -1990s ndash Primary cell IPG
bull 2004 ndash Rechargeable IPG
Clinical studies on SCS continue to support the effectiveness of this
therapy The following charts summarize studies of SCS and its
effects on the quality of life of patients
Reduction of Pain
ReferenceNumber of
PatientsFollow Up Results
Kumar17 410 8 years 74 had gt50 relief
North14 19 3 years 47 had gt50 relief
Barolat9 41 1 year50-65 had good to
excellent relief
Van Buyten18 123 3 years68 had good to excellent
relief
Cameron19 747Up to 59 months
(49 years)
62 had gt50 relief or
significantly reduced pain
scores
SCS indikaacutecioacutek INeuropaacutethiaacutes (neurogeacuten) faacutejdalom
bull Perifeacuteriaacutes idegek seacuteruumlleacutese gyoumlkoumlk plexusok (idegrendszeri hiaacutenytuumlnet) seacuteruumlleacutes okai baleseti műteacutet pl lumbaacutelis discectomia (gyoumlk) nőgyoacutegyaacuteszati (inguinalis ideg) teacuterdműteacutetek (infrapatellaacuteris ideg) mastectomia (costo-brachiaacutelis ideg)
bull veacutegtag-amputaacutecioacute csonkfaacutejdalom jobban mint a fantom faacutejdalombull post-herpeses neuralgia amennyiben a bőreacuterzeacutes reacuteszlegesen megtartottbull post-irradiaacutecioacutes plexopaacutetiabull polyneuropaacutetiaacutek (diabeteses alkoholos) post-kemoteraacutepiaacutes (amennyiben a vastag rostok
műkoumldeacutese reacuteszlegesen megtartott)bull gerincvelő incomplett seacuteruumlleacutese -amennyiben a vastag eacuterzőrostok műkoumldeacutese megtartott eacutes a
segmentaacutelis faacutejdalom a seacuteruumlleacutes magassaacutegaacuteban leacutep felbull cervicaacutelis eacutes lumbosacralis radiculopaacutetiaacutek (compresszioacute ischaemia sebeacuteszi baleset
arachnoiditisbull CRPS II (causalga)bull DE bull plexus avulsioacute syringomyelia faacutejdalom nem csillapiacutethatoacutek bull nincs egyeteacuterteacutes a CRPS I (reflex sympaticus dystrophia)
SCS indikaacutecioacutek II
bull Kevert faacutejdalom szindroacutemaacutek
Falied back surgery syndroma = FBSS koraacutebbi gerincsebeacuteszeti beavatkozaacutes (postoperatiacutev fibrosis arachnoiditis)
Posztlaminektomiaacutes szindroacutemaangolszaacutesz failed back surgery szindroacutemaacutenak (FBSS)
bull faacutejdalom lokalizaacutecioacute alsoacute aacutegyeacuteki gerinc far
alsoacute veacutegtagok
bull etioloacutegia arachnoiditis epiduraacutelis heg
radiculitis mikro-instabilitaacutes rec
porckorongseacuterv gyulladaacutes
bull tapasztalatok alsoacute veacutegtagba terjedő
faacutejdalomra SCS hateacutekony
bull axiaacutelis faacutejdalmakra nem bizonyiacutetott
Incidencia FBSS
bull ranges 5 - 50
bull postdiscectomy 10-40
Etiologia FBSS
bull Scar tissue that forms around the surgery site interrupting normal neurological functioning
bull technicalities of the operation are not successful the performing surgeon had poor technique andor there is iatrogenic injury present
bull surgery is not performed at the site that causes the pain
bull surgery performed is not actually necessarybull patient is a poor fit for a successful surgerybull diagnosis was incorrectbull Complications of surgery arise
1 Anderson VC et al Current review of pain 20004105-11 5 Vaccaro AR et al Spine 200126 (24) S111-82 Leveque JC et al Neuromodulation 200141-9 6 Spengler DM et al Spine 19805356-603 Dario A et al Neuromodulation 20014105-110 7 Fager CA Freidberg SR Spine 1980587-944 Ohnmeiss DD et al The Spine Journal 2001358-363 8 Long DM Surgical management of pain 2002 354-64
FBSS okai eacutes tuumlnetei
bull FBSS cause1-7
ndash irreversible nerve injury
ndash surgical complications
ndash psychosocial problems
ndash inappropriate selection of patients for surgery
ndash recurrent herniation
ndash wrong level of operation
bull FBSS symptoms348
ndash lumbosacral postoperative fibrosis andor arachnoiditis
ndash root lesion
ndash dorsal compartment syndrome
ndash lateral spinal stenosis
SCS indikaacutecioacutek IIIAngina pectoris
bull New York Heart Association III-IV csoport (szignifikaacutens coronaacuteria stenosis egy vagy toumlbb szűkuumllet 70 )
bull myocardiaacutelis ischaemia reverzibilis angina gyoacutegyszeres revascularizaacutecioacutes beavatkozaacutesokkal nem enyhiacutethető
bull eacuteletminőseacuteguarr nitro-glicerin felhasznaacutelaacutesdarr anginaacutes rohamok szaacutemadarr jaacuteraacutestaacutevolsaacuteguarr
bull SCS anti-ischaemiaacutes hataacutes
bull nincs bizonyiacuteteacutek SCS hateacutekonysaacutegra instabil angina acut myocardiaacutelis infarctus vazospasticus angia maacutes sziacutevbetegseacuteg okozta anginaacutes faacutejdalmak csillapiacutetaacutesaacutera
Anginaacutes faacutejdalom
SCS tanulmaacutenyok hateacutekonysaacuteg I
bull Nienke (45 ) PT 1 eacutev koumlveteacutes eacuteletminőseacuteg szociaacutelis mentaacutelis fizikaacutelis teljesiacutetmeacuteny szignifikaacutensan javul
bull Hautvast (46) stabil angina pectorisban RT 6 heacutet koumlveteacutes
Randomizaacutelaacutes a stimulaacutetor OFF b csoport 3x1 oacuteranap ON vagy hirtelen anginaacuteban
anginaacutes rohamszaacutem csoumlkken
fizikai teljesiacutetőkeacutepesseacuteg javul
sublinguaacutelis nitraacutet felhasznaacutelaacutes csoumlkken
EKG-n az ischaemiaacutes epizoacutedusok csoumlkkennek
ST depresszioacute enyhuumll eacuteletminőseacuteg javul
anginaacutes faacutejdalom csoumlkken
SCS indikaacutecioacutek IIIAngina pectoris
bull tanulmaacutenyok eredmeacutenyei kedvezőek (39-43)
bull teraacutepiaacutes hataacutes hosszuacute taacutevuacute
bull nitraacutet bevitel csoumlkkenthető
bull faacutejdalomcsillapiacutetoacute hataacutesuacute
bull sziacutevizom veacuterkeringeacutes javul
bull PET tanulmaacuteny
ischaemiaacutes sziacutevizomban keringeacuteseacuteben
redistribucio alakul ki nyugalomban
eacutes gyoacutegyszer indukaacutelt stresszben(44)
SCS indikaacutecioacutek IVPerifeacuteriaacutes vasculaacuteris betegseacutegek
bull lassan progrediaacuteloacute perifeacuteriaacutes vasculaacuteris ischaemia -atherosclerosis (Fontaine 3 4 staacutedium )
bull vazospasticus betegseacuteg (pl Raynaud frostbite) gyoacutegyszeresen eacutersebeacuteszeti műteacutettel nem uralhatoacute veacutegtagfaacutejdalom
bull Buerger-koacuter
bull kontraindikaacutelt laacutebszaacuterfekeacutelygt 3 cm gangreacutena
SCS indikaacutecioacutek VCRPS
CRPS tuumlnetei
1 Harden RN et al Pain 199983211-219 6Birklein F et al Pain 19976949-54
2 Galer BS et al J Pain Symptom Manage 200020286-92 7 Schwartzman RJ Kerrigan J
Neurosurgery 19904057-61
3 Birklein F Handwerker HO Pain 2001 941-6 8 Zyluk A J Hand Surg 200126151-154
4 Rommel O et al Pain 19998095-101 9 Wasner G et al Neuro Clin
199816851-68
5 Thimineur M et al Clin J Pain 199814256-67
Sensory Motor dysfunctionIntense pain12 Weakness
Allodynia13 Decreased range of motion3
Hyperesthesia13 Tremor16
Hyperalgesia13 Dystonia7
Sensory deficits4 Myoclonus7
Decreased muscular strength8
Autonomic Dystrophic Swelling1 Increaseddecreased nailhair growth
Colourtemperature changes6 Skin changes (eg palor plantar fibrosis
Sweating abnormalities6 hyperkeratosis and thin glossy
skin9 )
Courtesy of Robert J Schwartzman MD
SCS indikaacutecioacutek VIAbdominaacutelis eacutes visceraacutelis faacutejdalom
szindroacutemaacutek
bull Faacutejdalom etioloacutegiaacuteja vaacuteltozatos
bull Ok gastrointestinaacutelis gastro-urinaacutelis
musculosceletaacutelis idegrendszeri
bull Megfigyeleacutes Th X myelotomia
daganatos pelvicus faacutejdalmat csillapiacutet
Mechanisms of SCS
bull Gate control theory
bull Direct inhibition of spinothalamic neurons
bull Descending modulatory effects
bull Alteration of sympathetic activity
bull Neurochemical modulation
GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Neuromodulaacutecioacute
bull centraacutelis-perifeacuteriaacutes-autonom idegrendszer műkoumldeacuteseacutenek teraacutepiaacutes alteraacutecioacuteja
bull implantaacutelt keacuteszuumlleacutek
bull elektromos gyoacutegyszeres
bull non-destruktiacutev
bull reverzibilis
bull betegseacuteget nem gyoacutegyiacutet
bull műkoumldeacutest eacuteletminőseacuteget javiacutet
Neuromodulaacutecioacute tiacutepusai
bull Elektromos (neurostimulaacutecioacute)
bull Keacutemiai (gyoacutegyszerpumpa)
Neuropathic pain
bull International Association for the Study of Pain defines pain caused by a lesion or disease of the somatosensory nervous system
bull suffer more often from insomnia anxiety and depression1
bull analgetic medication insufficient2
bull SCS has undergone constant technical advancement
Why Neuromodulation
bull Testable
bull Completely reversible
bull Non-destructive
bull No limitation to future therapy
Neurostimulaacutecioacute helye
bull perifeacuteriaacutes ideg PNS PNfS DRGS
bull gerincvelő SCS
bull meacutelyagyi DBS
bull motoros agykeacutereg MCS
Neurostimulaacutecioacutes faacutejdalomcsillapiacutetoacute műteacutetek indikaacutecioacutejaacutenak felaacutelliacutetaacutesa
bull faacutejdalom kezeleacuteseacuteben jaacuteratos szakemberek koumlzoumls doumlnteacutese
bull centrumokban (kivizsgaacutelaacutes kezeleacutes szoumlvődmeacutenyek elhaacuteriacutetaacutesa)
bull multidisciplinaacuteris (ideggyoacutegyaacutesz idegsebeacutesz psychiaacuteter psycholoacutegus anaesthesioloacutegus neuroradioloacutegus elektrofizioloacutegus mozgaacutesterapeuta) munkacsoport
Neurostimulaacutecioacute aacuteltalaacutenos kontraindikaacutecioacutek
(kroacutenikus faacutejdalom)
bull psychiaacutetriai koacuterkeacutepek (aktiacutev psychosis suacutelyos depresszioacute hipochondria szomatizaacutecioacutes betegseacutegek)
bull nem egyuumlttműkoumldő beteg
bull alkoholizmus kaacutebiacutetoacuteszer-eacutelvezet
bull suacutelyos kiacuteseacuterő betegseacuteg (coagulopathia immundeficiencia)
bull maacutes implantaacutelt pacemaker (pl sziacutev)
Neurostimulaacutecioacute műteacuteti szoumlvődmeacutenyek
bull korrigaacutelhatoacutek
bull implantaacutetummal (8-10) kapcsolatos
(elektroacuteda elmozdulaacutes seacuteruumlleacutes elektromos műkoumldeacutes zavar)
bull veacuterzeacutesek (1-5)
bull gyulladaacutesok (5-7)
Spinal cord stimulaacutecioacute (SCS)
bull Legneacutepszerűbb leggyakrabban alkalmazott
bull Első SCS daganatos faacutejdalom (Shealey 1967)
History of Spinal Cord StimulationShealy 1969
bull 1967 ndash Long and Wall PNS
bull 1969 ndash Shealy SCS in humans
bull 1975 ndash Dooley perc electrode
bull Mid 1970s ndash self-powered battery
bull 1980s - programmable quad electrode
bull 1980s -1990s ndash Primary cell IPG
bull 2004 ndash Rechargeable IPG
Clinical studies on SCS continue to support the effectiveness of this
therapy The following charts summarize studies of SCS and its
effects on the quality of life of patients
Reduction of Pain
ReferenceNumber of
PatientsFollow Up Results
Kumar17 410 8 years 74 had gt50 relief
North14 19 3 years 47 had gt50 relief
Barolat9 41 1 year50-65 had good to
excellent relief
Van Buyten18 123 3 years68 had good to excellent
relief
Cameron19 747Up to 59 months
(49 years)
62 had gt50 relief or
significantly reduced pain
scores
SCS indikaacutecioacutek INeuropaacutethiaacutes (neurogeacuten) faacutejdalom
bull Perifeacuteriaacutes idegek seacuteruumlleacutese gyoumlkoumlk plexusok (idegrendszeri hiaacutenytuumlnet) seacuteruumlleacutes okai baleseti műteacutet pl lumbaacutelis discectomia (gyoumlk) nőgyoacutegyaacuteszati (inguinalis ideg) teacuterdműteacutetek (infrapatellaacuteris ideg) mastectomia (costo-brachiaacutelis ideg)
bull veacutegtag-amputaacutecioacute csonkfaacutejdalom jobban mint a fantom faacutejdalombull post-herpeses neuralgia amennyiben a bőreacuterzeacutes reacuteszlegesen megtartottbull post-irradiaacutecioacutes plexopaacutetiabull polyneuropaacutetiaacutek (diabeteses alkoholos) post-kemoteraacutepiaacutes (amennyiben a vastag rostok
műkoumldeacutese reacuteszlegesen megtartott)bull gerincvelő incomplett seacuteruumlleacutese -amennyiben a vastag eacuterzőrostok műkoumldeacutese megtartott eacutes a
segmentaacutelis faacutejdalom a seacuteruumlleacutes magassaacutegaacuteban leacutep felbull cervicaacutelis eacutes lumbosacralis radiculopaacutetiaacutek (compresszioacute ischaemia sebeacuteszi baleset
arachnoiditisbull CRPS II (causalga)bull DE bull plexus avulsioacute syringomyelia faacutejdalom nem csillapiacutethatoacutek bull nincs egyeteacuterteacutes a CRPS I (reflex sympaticus dystrophia)
SCS indikaacutecioacutek II
bull Kevert faacutejdalom szindroacutemaacutek
Falied back surgery syndroma = FBSS koraacutebbi gerincsebeacuteszeti beavatkozaacutes (postoperatiacutev fibrosis arachnoiditis)
Posztlaminektomiaacutes szindroacutemaangolszaacutesz failed back surgery szindroacutemaacutenak (FBSS)
bull faacutejdalom lokalizaacutecioacute alsoacute aacutegyeacuteki gerinc far
alsoacute veacutegtagok
bull etioloacutegia arachnoiditis epiduraacutelis heg
radiculitis mikro-instabilitaacutes rec
porckorongseacuterv gyulladaacutes
bull tapasztalatok alsoacute veacutegtagba terjedő
faacutejdalomra SCS hateacutekony
bull axiaacutelis faacutejdalmakra nem bizonyiacutetott
Incidencia FBSS
bull ranges 5 - 50
bull postdiscectomy 10-40
Etiologia FBSS
bull Scar tissue that forms around the surgery site interrupting normal neurological functioning
bull technicalities of the operation are not successful the performing surgeon had poor technique andor there is iatrogenic injury present
bull surgery is not performed at the site that causes the pain
bull surgery performed is not actually necessarybull patient is a poor fit for a successful surgerybull diagnosis was incorrectbull Complications of surgery arise
1 Anderson VC et al Current review of pain 20004105-11 5 Vaccaro AR et al Spine 200126 (24) S111-82 Leveque JC et al Neuromodulation 200141-9 6 Spengler DM et al Spine 19805356-603 Dario A et al Neuromodulation 20014105-110 7 Fager CA Freidberg SR Spine 1980587-944 Ohnmeiss DD et al The Spine Journal 2001358-363 8 Long DM Surgical management of pain 2002 354-64
FBSS okai eacutes tuumlnetei
bull FBSS cause1-7
ndash irreversible nerve injury
ndash surgical complications
ndash psychosocial problems
ndash inappropriate selection of patients for surgery
ndash recurrent herniation
ndash wrong level of operation
bull FBSS symptoms348
ndash lumbosacral postoperative fibrosis andor arachnoiditis
ndash root lesion
ndash dorsal compartment syndrome
ndash lateral spinal stenosis
SCS indikaacutecioacutek IIIAngina pectoris
bull New York Heart Association III-IV csoport (szignifikaacutens coronaacuteria stenosis egy vagy toumlbb szűkuumllet 70 )
bull myocardiaacutelis ischaemia reverzibilis angina gyoacutegyszeres revascularizaacutecioacutes beavatkozaacutesokkal nem enyhiacutethető
bull eacuteletminőseacuteguarr nitro-glicerin felhasznaacutelaacutesdarr anginaacutes rohamok szaacutemadarr jaacuteraacutestaacutevolsaacuteguarr
bull SCS anti-ischaemiaacutes hataacutes
bull nincs bizonyiacuteteacutek SCS hateacutekonysaacutegra instabil angina acut myocardiaacutelis infarctus vazospasticus angia maacutes sziacutevbetegseacuteg okozta anginaacutes faacutejdalmak csillapiacutetaacutesaacutera
Anginaacutes faacutejdalom
SCS tanulmaacutenyok hateacutekonysaacuteg I
bull Nienke (45 ) PT 1 eacutev koumlveteacutes eacuteletminőseacuteg szociaacutelis mentaacutelis fizikaacutelis teljesiacutetmeacuteny szignifikaacutensan javul
bull Hautvast (46) stabil angina pectorisban RT 6 heacutet koumlveteacutes
Randomizaacutelaacutes a stimulaacutetor OFF b csoport 3x1 oacuteranap ON vagy hirtelen anginaacuteban
anginaacutes rohamszaacutem csoumlkken
fizikai teljesiacutetőkeacutepesseacuteg javul
sublinguaacutelis nitraacutet felhasznaacutelaacutes csoumlkken
EKG-n az ischaemiaacutes epizoacutedusok csoumlkkennek
ST depresszioacute enyhuumll eacuteletminőseacuteg javul
anginaacutes faacutejdalom csoumlkken
SCS indikaacutecioacutek IIIAngina pectoris
bull tanulmaacutenyok eredmeacutenyei kedvezőek (39-43)
bull teraacutepiaacutes hataacutes hosszuacute taacutevuacute
bull nitraacutet bevitel csoumlkkenthető
bull faacutejdalomcsillapiacutetoacute hataacutesuacute
bull sziacutevizom veacuterkeringeacutes javul
bull PET tanulmaacuteny
ischaemiaacutes sziacutevizomban keringeacuteseacuteben
redistribucio alakul ki nyugalomban
eacutes gyoacutegyszer indukaacutelt stresszben(44)
SCS indikaacutecioacutek IVPerifeacuteriaacutes vasculaacuteris betegseacutegek
bull lassan progrediaacuteloacute perifeacuteriaacutes vasculaacuteris ischaemia -atherosclerosis (Fontaine 3 4 staacutedium )
bull vazospasticus betegseacuteg (pl Raynaud frostbite) gyoacutegyszeresen eacutersebeacuteszeti műteacutettel nem uralhatoacute veacutegtagfaacutejdalom
bull Buerger-koacuter
bull kontraindikaacutelt laacutebszaacuterfekeacutelygt 3 cm gangreacutena
SCS indikaacutecioacutek VCRPS
CRPS tuumlnetei
1 Harden RN et al Pain 199983211-219 6Birklein F et al Pain 19976949-54
2 Galer BS et al J Pain Symptom Manage 200020286-92 7 Schwartzman RJ Kerrigan J
Neurosurgery 19904057-61
3 Birklein F Handwerker HO Pain 2001 941-6 8 Zyluk A J Hand Surg 200126151-154
4 Rommel O et al Pain 19998095-101 9 Wasner G et al Neuro Clin
199816851-68
5 Thimineur M et al Clin J Pain 199814256-67
Sensory Motor dysfunctionIntense pain12 Weakness
Allodynia13 Decreased range of motion3
Hyperesthesia13 Tremor16
Hyperalgesia13 Dystonia7
Sensory deficits4 Myoclonus7
Decreased muscular strength8
Autonomic Dystrophic Swelling1 Increaseddecreased nailhair growth
Colourtemperature changes6 Skin changes (eg palor plantar fibrosis
Sweating abnormalities6 hyperkeratosis and thin glossy
skin9 )
Courtesy of Robert J Schwartzman MD
SCS indikaacutecioacutek VIAbdominaacutelis eacutes visceraacutelis faacutejdalom
szindroacutemaacutek
bull Faacutejdalom etioloacutegiaacuteja vaacuteltozatos
bull Ok gastrointestinaacutelis gastro-urinaacutelis
musculosceletaacutelis idegrendszeri
bull Megfigyeleacutes Th X myelotomia
daganatos pelvicus faacutejdalmat csillapiacutet
Mechanisms of SCS
bull Gate control theory
bull Direct inhibition of spinothalamic neurons
bull Descending modulatory effects
bull Alteration of sympathetic activity
bull Neurochemical modulation
GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Neuromodulaacutecioacute tiacutepusai
bull Elektromos (neurostimulaacutecioacute)
bull Keacutemiai (gyoacutegyszerpumpa)
Neuropathic pain
bull International Association for the Study of Pain defines pain caused by a lesion or disease of the somatosensory nervous system
bull suffer more often from insomnia anxiety and depression1
bull analgetic medication insufficient2
bull SCS has undergone constant technical advancement
Why Neuromodulation
bull Testable
bull Completely reversible
bull Non-destructive
bull No limitation to future therapy
Neurostimulaacutecioacute helye
bull perifeacuteriaacutes ideg PNS PNfS DRGS
bull gerincvelő SCS
bull meacutelyagyi DBS
bull motoros agykeacutereg MCS
Neurostimulaacutecioacutes faacutejdalomcsillapiacutetoacute műteacutetek indikaacutecioacutejaacutenak felaacutelliacutetaacutesa
bull faacutejdalom kezeleacuteseacuteben jaacuteratos szakemberek koumlzoumls doumlnteacutese
bull centrumokban (kivizsgaacutelaacutes kezeleacutes szoumlvődmeacutenyek elhaacuteriacutetaacutesa)
bull multidisciplinaacuteris (ideggyoacutegyaacutesz idegsebeacutesz psychiaacuteter psycholoacutegus anaesthesioloacutegus neuroradioloacutegus elektrofizioloacutegus mozgaacutesterapeuta) munkacsoport
Neurostimulaacutecioacute aacuteltalaacutenos kontraindikaacutecioacutek
(kroacutenikus faacutejdalom)
bull psychiaacutetriai koacuterkeacutepek (aktiacutev psychosis suacutelyos depresszioacute hipochondria szomatizaacutecioacutes betegseacutegek)
bull nem egyuumlttműkoumldő beteg
bull alkoholizmus kaacutebiacutetoacuteszer-eacutelvezet
bull suacutelyos kiacuteseacuterő betegseacuteg (coagulopathia immundeficiencia)
bull maacutes implantaacutelt pacemaker (pl sziacutev)
Neurostimulaacutecioacute műteacuteti szoumlvődmeacutenyek
bull korrigaacutelhatoacutek
bull implantaacutetummal (8-10) kapcsolatos
(elektroacuteda elmozdulaacutes seacuteruumlleacutes elektromos műkoumldeacutes zavar)
bull veacuterzeacutesek (1-5)
bull gyulladaacutesok (5-7)
Spinal cord stimulaacutecioacute (SCS)
bull Legneacutepszerűbb leggyakrabban alkalmazott
bull Első SCS daganatos faacutejdalom (Shealey 1967)
History of Spinal Cord StimulationShealy 1969
bull 1967 ndash Long and Wall PNS
bull 1969 ndash Shealy SCS in humans
bull 1975 ndash Dooley perc electrode
bull Mid 1970s ndash self-powered battery
bull 1980s - programmable quad electrode
bull 1980s -1990s ndash Primary cell IPG
bull 2004 ndash Rechargeable IPG
Clinical studies on SCS continue to support the effectiveness of this
therapy The following charts summarize studies of SCS and its
effects on the quality of life of patients
Reduction of Pain
ReferenceNumber of
PatientsFollow Up Results
Kumar17 410 8 years 74 had gt50 relief
North14 19 3 years 47 had gt50 relief
Barolat9 41 1 year50-65 had good to
excellent relief
Van Buyten18 123 3 years68 had good to excellent
relief
Cameron19 747Up to 59 months
(49 years)
62 had gt50 relief or
significantly reduced pain
scores
SCS indikaacutecioacutek INeuropaacutethiaacutes (neurogeacuten) faacutejdalom
bull Perifeacuteriaacutes idegek seacuteruumlleacutese gyoumlkoumlk plexusok (idegrendszeri hiaacutenytuumlnet) seacuteruumlleacutes okai baleseti műteacutet pl lumbaacutelis discectomia (gyoumlk) nőgyoacutegyaacuteszati (inguinalis ideg) teacuterdműteacutetek (infrapatellaacuteris ideg) mastectomia (costo-brachiaacutelis ideg)
bull veacutegtag-amputaacutecioacute csonkfaacutejdalom jobban mint a fantom faacutejdalombull post-herpeses neuralgia amennyiben a bőreacuterzeacutes reacuteszlegesen megtartottbull post-irradiaacutecioacutes plexopaacutetiabull polyneuropaacutetiaacutek (diabeteses alkoholos) post-kemoteraacutepiaacutes (amennyiben a vastag rostok
műkoumldeacutese reacuteszlegesen megtartott)bull gerincvelő incomplett seacuteruumlleacutese -amennyiben a vastag eacuterzőrostok műkoumldeacutese megtartott eacutes a
segmentaacutelis faacutejdalom a seacuteruumlleacutes magassaacutegaacuteban leacutep felbull cervicaacutelis eacutes lumbosacralis radiculopaacutetiaacutek (compresszioacute ischaemia sebeacuteszi baleset
arachnoiditisbull CRPS II (causalga)bull DE bull plexus avulsioacute syringomyelia faacutejdalom nem csillapiacutethatoacutek bull nincs egyeteacuterteacutes a CRPS I (reflex sympaticus dystrophia)
SCS indikaacutecioacutek II
bull Kevert faacutejdalom szindroacutemaacutek
Falied back surgery syndroma = FBSS koraacutebbi gerincsebeacuteszeti beavatkozaacutes (postoperatiacutev fibrosis arachnoiditis)
Posztlaminektomiaacutes szindroacutemaangolszaacutesz failed back surgery szindroacutemaacutenak (FBSS)
bull faacutejdalom lokalizaacutecioacute alsoacute aacutegyeacuteki gerinc far
alsoacute veacutegtagok
bull etioloacutegia arachnoiditis epiduraacutelis heg
radiculitis mikro-instabilitaacutes rec
porckorongseacuterv gyulladaacutes
bull tapasztalatok alsoacute veacutegtagba terjedő
faacutejdalomra SCS hateacutekony
bull axiaacutelis faacutejdalmakra nem bizonyiacutetott
Incidencia FBSS
bull ranges 5 - 50
bull postdiscectomy 10-40
Etiologia FBSS
bull Scar tissue that forms around the surgery site interrupting normal neurological functioning
bull technicalities of the operation are not successful the performing surgeon had poor technique andor there is iatrogenic injury present
bull surgery is not performed at the site that causes the pain
bull surgery performed is not actually necessarybull patient is a poor fit for a successful surgerybull diagnosis was incorrectbull Complications of surgery arise
1 Anderson VC et al Current review of pain 20004105-11 5 Vaccaro AR et al Spine 200126 (24) S111-82 Leveque JC et al Neuromodulation 200141-9 6 Spengler DM et al Spine 19805356-603 Dario A et al Neuromodulation 20014105-110 7 Fager CA Freidberg SR Spine 1980587-944 Ohnmeiss DD et al The Spine Journal 2001358-363 8 Long DM Surgical management of pain 2002 354-64
FBSS okai eacutes tuumlnetei
bull FBSS cause1-7
ndash irreversible nerve injury
ndash surgical complications
ndash psychosocial problems
ndash inappropriate selection of patients for surgery
ndash recurrent herniation
ndash wrong level of operation
bull FBSS symptoms348
ndash lumbosacral postoperative fibrosis andor arachnoiditis
ndash root lesion
ndash dorsal compartment syndrome
ndash lateral spinal stenosis
SCS indikaacutecioacutek IIIAngina pectoris
bull New York Heart Association III-IV csoport (szignifikaacutens coronaacuteria stenosis egy vagy toumlbb szűkuumllet 70 )
bull myocardiaacutelis ischaemia reverzibilis angina gyoacutegyszeres revascularizaacutecioacutes beavatkozaacutesokkal nem enyhiacutethető
bull eacuteletminőseacuteguarr nitro-glicerin felhasznaacutelaacutesdarr anginaacutes rohamok szaacutemadarr jaacuteraacutestaacutevolsaacuteguarr
bull SCS anti-ischaemiaacutes hataacutes
bull nincs bizonyiacuteteacutek SCS hateacutekonysaacutegra instabil angina acut myocardiaacutelis infarctus vazospasticus angia maacutes sziacutevbetegseacuteg okozta anginaacutes faacutejdalmak csillapiacutetaacutesaacutera
Anginaacutes faacutejdalom
SCS tanulmaacutenyok hateacutekonysaacuteg I
bull Nienke (45 ) PT 1 eacutev koumlveteacutes eacuteletminőseacuteg szociaacutelis mentaacutelis fizikaacutelis teljesiacutetmeacuteny szignifikaacutensan javul
bull Hautvast (46) stabil angina pectorisban RT 6 heacutet koumlveteacutes
Randomizaacutelaacutes a stimulaacutetor OFF b csoport 3x1 oacuteranap ON vagy hirtelen anginaacuteban
anginaacutes rohamszaacutem csoumlkken
fizikai teljesiacutetőkeacutepesseacuteg javul
sublinguaacutelis nitraacutet felhasznaacutelaacutes csoumlkken
EKG-n az ischaemiaacutes epizoacutedusok csoumlkkennek
ST depresszioacute enyhuumll eacuteletminőseacuteg javul
anginaacutes faacutejdalom csoumlkken
SCS indikaacutecioacutek IIIAngina pectoris
bull tanulmaacutenyok eredmeacutenyei kedvezőek (39-43)
bull teraacutepiaacutes hataacutes hosszuacute taacutevuacute
bull nitraacutet bevitel csoumlkkenthető
bull faacutejdalomcsillapiacutetoacute hataacutesuacute
bull sziacutevizom veacuterkeringeacutes javul
bull PET tanulmaacuteny
ischaemiaacutes sziacutevizomban keringeacuteseacuteben
redistribucio alakul ki nyugalomban
eacutes gyoacutegyszer indukaacutelt stresszben(44)
SCS indikaacutecioacutek IVPerifeacuteriaacutes vasculaacuteris betegseacutegek
bull lassan progrediaacuteloacute perifeacuteriaacutes vasculaacuteris ischaemia -atherosclerosis (Fontaine 3 4 staacutedium )
bull vazospasticus betegseacuteg (pl Raynaud frostbite) gyoacutegyszeresen eacutersebeacuteszeti műteacutettel nem uralhatoacute veacutegtagfaacutejdalom
bull Buerger-koacuter
bull kontraindikaacutelt laacutebszaacuterfekeacutelygt 3 cm gangreacutena
SCS indikaacutecioacutek VCRPS
CRPS tuumlnetei
1 Harden RN et al Pain 199983211-219 6Birklein F et al Pain 19976949-54
2 Galer BS et al J Pain Symptom Manage 200020286-92 7 Schwartzman RJ Kerrigan J
Neurosurgery 19904057-61
3 Birklein F Handwerker HO Pain 2001 941-6 8 Zyluk A J Hand Surg 200126151-154
4 Rommel O et al Pain 19998095-101 9 Wasner G et al Neuro Clin
199816851-68
5 Thimineur M et al Clin J Pain 199814256-67
Sensory Motor dysfunctionIntense pain12 Weakness
Allodynia13 Decreased range of motion3
Hyperesthesia13 Tremor16
Hyperalgesia13 Dystonia7
Sensory deficits4 Myoclonus7
Decreased muscular strength8
Autonomic Dystrophic Swelling1 Increaseddecreased nailhair growth
Colourtemperature changes6 Skin changes (eg palor plantar fibrosis
Sweating abnormalities6 hyperkeratosis and thin glossy
skin9 )
Courtesy of Robert J Schwartzman MD
SCS indikaacutecioacutek VIAbdominaacutelis eacutes visceraacutelis faacutejdalom
szindroacutemaacutek
bull Faacutejdalom etioloacutegiaacuteja vaacuteltozatos
bull Ok gastrointestinaacutelis gastro-urinaacutelis
musculosceletaacutelis idegrendszeri
bull Megfigyeleacutes Th X myelotomia
daganatos pelvicus faacutejdalmat csillapiacutet
Mechanisms of SCS
bull Gate control theory
bull Direct inhibition of spinothalamic neurons
bull Descending modulatory effects
bull Alteration of sympathetic activity
bull Neurochemical modulation
GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Neuropathic pain
bull International Association for the Study of Pain defines pain caused by a lesion or disease of the somatosensory nervous system
bull suffer more often from insomnia anxiety and depression1
bull analgetic medication insufficient2
bull SCS has undergone constant technical advancement
Why Neuromodulation
bull Testable
bull Completely reversible
bull Non-destructive
bull No limitation to future therapy
Neurostimulaacutecioacute helye
bull perifeacuteriaacutes ideg PNS PNfS DRGS
bull gerincvelő SCS
bull meacutelyagyi DBS
bull motoros agykeacutereg MCS
Neurostimulaacutecioacutes faacutejdalomcsillapiacutetoacute műteacutetek indikaacutecioacutejaacutenak felaacutelliacutetaacutesa
bull faacutejdalom kezeleacuteseacuteben jaacuteratos szakemberek koumlzoumls doumlnteacutese
bull centrumokban (kivizsgaacutelaacutes kezeleacutes szoumlvődmeacutenyek elhaacuteriacutetaacutesa)
bull multidisciplinaacuteris (ideggyoacutegyaacutesz idegsebeacutesz psychiaacuteter psycholoacutegus anaesthesioloacutegus neuroradioloacutegus elektrofizioloacutegus mozgaacutesterapeuta) munkacsoport
Neurostimulaacutecioacute aacuteltalaacutenos kontraindikaacutecioacutek
(kroacutenikus faacutejdalom)
bull psychiaacutetriai koacuterkeacutepek (aktiacutev psychosis suacutelyos depresszioacute hipochondria szomatizaacutecioacutes betegseacutegek)
bull nem egyuumlttműkoumldő beteg
bull alkoholizmus kaacutebiacutetoacuteszer-eacutelvezet
bull suacutelyos kiacuteseacuterő betegseacuteg (coagulopathia immundeficiencia)
bull maacutes implantaacutelt pacemaker (pl sziacutev)
Neurostimulaacutecioacute műteacuteti szoumlvődmeacutenyek
bull korrigaacutelhatoacutek
bull implantaacutetummal (8-10) kapcsolatos
(elektroacuteda elmozdulaacutes seacuteruumlleacutes elektromos műkoumldeacutes zavar)
bull veacuterzeacutesek (1-5)
bull gyulladaacutesok (5-7)
Spinal cord stimulaacutecioacute (SCS)
bull Legneacutepszerűbb leggyakrabban alkalmazott
bull Első SCS daganatos faacutejdalom (Shealey 1967)
History of Spinal Cord StimulationShealy 1969
bull 1967 ndash Long and Wall PNS
bull 1969 ndash Shealy SCS in humans
bull 1975 ndash Dooley perc electrode
bull Mid 1970s ndash self-powered battery
bull 1980s - programmable quad electrode
bull 1980s -1990s ndash Primary cell IPG
bull 2004 ndash Rechargeable IPG
Clinical studies on SCS continue to support the effectiveness of this
therapy The following charts summarize studies of SCS and its
effects on the quality of life of patients
Reduction of Pain
ReferenceNumber of
PatientsFollow Up Results
Kumar17 410 8 years 74 had gt50 relief
North14 19 3 years 47 had gt50 relief
Barolat9 41 1 year50-65 had good to
excellent relief
Van Buyten18 123 3 years68 had good to excellent
relief
Cameron19 747Up to 59 months
(49 years)
62 had gt50 relief or
significantly reduced pain
scores
SCS indikaacutecioacutek INeuropaacutethiaacutes (neurogeacuten) faacutejdalom
bull Perifeacuteriaacutes idegek seacuteruumlleacutese gyoumlkoumlk plexusok (idegrendszeri hiaacutenytuumlnet) seacuteruumlleacutes okai baleseti műteacutet pl lumbaacutelis discectomia (gyoumlk) nőgyoacutegyaacuteszati (inguinalis ideg) teacuterdműteacutetek (infrapatellaacuteris ideg) mastectomia (costo-brachiaacutelis ideg)
bull veacutegtag-amputaacutecioacute csonkfaacutejdalom jobban mint a fantom faacutejdalombull post-herpeses neuralgia amennyiben a bőreacuterzeacutes reacuteszlegesen megtartottbull post-irradiaacutecioacutes plexopaacutetiabull polyneuropaacutetiaacutek (diabeteses alkoholos) post-kemoteraacutepiaacutes (amennyiben a vastag rostok
műkoumldeacutese reacuteszlegesen megtartott)bull gerincvelő incomplett seacuteruumlleacutese -amennyiben a vastag eacuterzőrostok műkoumldeacutese megtartott eacutes a
segmentaacutelis faacutejdalom a seacuteruumlleacutes magassaacutegaacuteban leacutep felbull cervicaacutelis eacutes lumbosacralis radiculopaacutetiaacutek (compresszioacute ischaemia sebeacuteszi baleset
arachnoiditisbull CRPS II (causalga)bull DE bull plexus avulsioacute syringomyelia faacutejdalom nem csillapiacutethatoacutek bull nincs egyeteacuterteacutes a CRPS I (reflex sympaticus dystrophia)
SCS indikaacutecioacutek II
bull Kevert faacutejdalom szindroacutemaacutek
Falied back surgery syndroma = FBSS koraacutebbi gerincsebeacuteszeti beavatkozaacutes (postoperatiacutev fibrosis arachnoiditis)
Posztlaminektomiaacutes szindroacutemaangolszaacutesz failed back surgery szindroacutemaacutenak (FBSS)
bull faacutejdalom lokalizaacutecioacute alsoacute aacutegyeacuteki gerinc far
alsoacute veacutegtagok
bull etioloacutegia arachnoiditis epiduraacutelis heg
radiculitis mikro-instabilitaacutes rec
porckorongseacuterv gyulladaacutes
bull tapasztalatok alsoacute veacutegtagba terjedő
faacutejdalomra SCS hateacutekony
bull axiaacutelis faacutejdalmakra nem bizonyiacutetott
Incidencia FBSS
bull ranges 5 - 50
bull postdiscectomy 10-40
Etiologia FBSS
bull Scar tissue that forms around the surgery site interrupting normal neurological functioning
bull technicalities of the operation are not successful the performing surgeon had poor technique andor there is iatrogenic injury present
bull surgery is not performed at the site that causes the pain
bull surgery performed is not actually necessarybull patient is a poor fit for a successful surgerybull diagnosis was incorrectbull Complications of surgery arise
1 Anderson VC et al Current review of pain 20004105-11 5 Vaccaro AR et al Spine 200126 (24) S111-82 Leveque JC et al Neuromodulation 200141-9 6 Spengler DM et al Spine 19805356-603 Dario A et al Neuromodulation 20014105-110 7 Fager CA Freidberg SR Spine 1980587-944 Ohnmeiss DD et al The Spine Journal 2001358-363 8 Long DM Surgical management of pain 2002 354-64
FBSS okai eacutes tuumlnetei
bull FBSS cause1-7
ndash irreversible nerve injury
ndash surgical complications
ndash psychosocial problems
ndash inappropriate selection of patients for surgery
ndash recurrent herniation
ndash wrong level of operation
bull FBSS symptoms348
ndash lumbosacral postoperative fibrosis andor arachnoiditis
ndash root lesion
ndash dorsal compartment syndrome
ndash lateral spinal stenosis
SCS indikaacutecioacutek IIIAngina pectoris
bull New York Heart Association III-IV csoport (szignifikaacutens coronaacuteria stenosis egy vagy toumlbb szűkuumllet 70 )
bull myocardiaacutelis ischaemia reverzibilis angina gyoacutegyszeres revascularizaacutecioacutes beavatkozaacutesokkal nem enyhiacutethető
bull eacuteletminőseacuteguarr nitro-glicerin felhasznaacutelaacutesdarr anginaacutes rohamok szaacutemadarr jaacuteraacutestaacutevolsaacuteguarr
bull SCS anti-ischaemiaacutes hataacutes
bull nincs bizonyiacuteteacutek SCS hateacutekonysaacutegra instabil angina acut myocardiaacutelis infarctus vazospasticus angia maacutes sziacutevbetegseacuteg okozta anginaacutes faacutejdalmak csillapiacutetaacutesaacutera
Anginaacutes faacutejdalom
SCS tanulmaacutenyok hateacutekonysaacuteg I
bull Nienke (45 ) PT 1 eacutev koumlveteacutes eacuteletminőseacuteg szociaacutelis mentaacutelis fizikaacutelis teljesiacutetmeacuteny szignifikaacutensan javul
bull Hautvast (46) stabil angina pectorisban RT 6 heacutet koumlveteacutes
Randomizaacutelaacutes a stimulaacutetor OFF b csoport 3x1 oacuteranap ON vagy hirtelen anginaacuteban
anginaacutes rohamszaacutem csoumlkken
fizikai teljesiacutetőkeacutepesseacuteg javul
sublinguaacutelis nitraacutet felhasznaacutelaacutes csoumlkken
EKG-n az ischaemiaacutes epizoacutedusok csoumlkkennek
ST depresszioacute enyhuumll eacuteletminőseacuteg javul
anginaacutes faacutejdalom csoumlkken
SCS indikaacutecioacutek IIIAngina pectoris
bull tanulmaacutenyok eredmeacutenyei kedvezőek (39-43)
bull teraacutepiaacutes hataacutes hosszuacute taacutevuacute
bull nitraacutet bevitel csoumlkkenthető
bull faacutejdalomcsillapiacutetoacute hataacutesuacute
bull sziacutevizom veacuterkeringeacutes javul
bull PET tanulmaacuteny
ischaemiaacutes sziacutevizomban keringeacuteseacuteben
redistribucio alakul ki nyugalomban
eacutes gyoacutegyszer indukaacutelt stresszben(44)
SCS indikaacutecioacutek IVPerifeacuteriaacutes vasculaacuteris betegseacutegek
bull lassan progrediaacuteloacute perifeacuteriaacutes vasculaacuteris ischaemia -atherosclerosis (Fontaine 3 4 staacutedium )
bull vazospasticus betegseacuteg (pl Raynaud frostbite) gyoacutegyszeresen eacutersebeacuteszeti műteacutettel nem uralhatoacute veacutegtagfaacutejdalom
bull Buerger-koacuter
bull kontraindikaacutelt laacutebszaacuterfekeacutelygt 3 cm gangreacutena
SCS indikaacutecioacutek VCRPS
CRPS tuumlnetei
1 Harden RN et al Pain 199983211-219 6Birklein F et al Pain 19976949-54
2 Galer BS et al J Pain Symptom Manage 200020286-92 7 Schwartzman RJ Kerrigan J
Neurosurgery 19904057-61
3 Birklein F Handwerker HO Pain 2001 941-6 8 Zyluk A J Hand Surg 200126151-154
4 Rommel O et al Pain 19998095-101 9 Wasner G et al Neuro Clin
199816851-68
5 Thimineur M et al Clin J Pain 199814256-67
Sensory Motor dysfunctionIntense pain12 Weakness
Allodynia13 Decreased range of motion3
Hyperesthesia13 Tremor16
Hyperalgesia13 Dystonia7
Sensory deficits4 Myoclonus7
Decreased muscular strength8
Autonomic Dystrophic Swelling1 Increaseddecreased nailhair growth
Colourtemperature changes6 Skin changes (eg palor plantar fibrosis
Sweating abnormalities6 hyperkeratosis and thin glossy
skin9 )
Courtesy of Robert J Schwartzman MD
SCS indikaacutecioacutek VIAbdominaacutelis eacutes visceraacutelis faacutejdalom
szindroacutemaacutek
bull Faacutejdalom etioloacutegiaacuteja vaacuteltozatos
bull Ok gastrointestinaacutelis gastro-urinaacutelis
musculosceletaacutelis idegrendszeri
bull Megfigyeleacutes Th X myelotomia
daganatos pelvicus faacutejdalmat csillapiacutet
Mechanisms of SCS
bull Gate control theory
bull Direct inhibition of spinothalamic neurons
bull Descending modulatory effects
bull Alteration of sympathetic activity
bull Neurochemical modulation
GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Why Neuromodulation
bull Testable
bull Completely reversible
bull Non-destructive
bull No limitation to future therapy
Neurostimulaacutecioacute helye
bull perifeacuteriaacutes ideg PNS PNfS DRGS
bull gerincvelő SCS
bull meacutelyagyi DBS
bull motoros agykeacutereg MCS
Neurostimulaacutecioacutes faacutejdalomcsillapiacutetoacute műteacutetek indikaacutecioacutejaacutenak felaacutelliacutetaacutesa
bull faacutejdalom kezeleacuteseacuteben jaacuteratos szakemberek koumlzoumls doumlnteacutese
bull centrumokban (kivizsgaacutelaacutes kezeleacutes szoumlvődmeacutenyek elhaacuteriacutetaacutesa)
bull multidisciplinaacuteris (ideggyoacutegyaacutesz idegsebeacutesz psychiaacuteter psycholoacutegus anaesthesioloacutegus neuroradioloacutegus elektrofizioloacutegus mozgaacutesterapeuta) munkacsoport
Neurostimulaacutecioacute aacuteltalaacutenos kontraindikaacutecioacutek
(kroacutenikus faacutejdalom)
bull psychiaacutetriai koacuterkeacutepek (aktiacutev psychosis suacutelyos depresszioacute hipochondria szomatizaacutecioacutes betegseacutegek)
bull nem egyuumlttműkoumldő beteg
bull alkoholizmus kaacutebiacutetoacuteszer-eacutelvezet
bull suacutelyos kiacuteseacuterő betegseacuteg (coagulopathia immundeficiencia)
bull maacutes implantaacutelt pacemaker (pl sziacutev)
Neurostimulaacutecioacute műteacuteti szoumlvődmeacutenyek
bull korrigaacutelhatoacutek
bull implantaacutetummal (8-10) kapcsolatos
(elektroacuteda elmozdulaacutes seacuteruumlleacutes elektromos műkoumldeacutes zavar)
bull veacuterzeacutesek (1-5)
bull gyulladaacutesok (5-7)
Spinal cord stimulaacutecioacute (SCS)
bull Legneacutepszerűbb leggyakrabban alkalmazott
bull Első SCS daganatos faacutejdalom (Shealey 1967)
History of Spinal Cord StimulationShealy 1969
bull 1967 ndash Long and Wall PNS
bull 1969 ndash Shealy SCS in humans
bull 1975 ndash Dooley perc electrode
bull Mid 1970s ndash self-powered battery
bull 1980s - programmable quad electrode
bull 1980s -1990s ndash Primary cell IPG
bull 2004 ndash Rechargeable IPG
Clinical studies on SCS continue to support the effectiveness of this
therapy The following charts summarize studies of SCS and its
effects on the quality of life of patients
Reduction of Pain
ReferenceNumber of
PatientsFollow Up Results
Kumar17 410 8 years 74 had gt50 relief
North14 19 3 years 47 had gt50 relief
Barolat9 41 1 year50-65 had good to
excellent relief
Van Buyten18 123 3 years68 had good to excellent
relief
Cameron19 747Up to 59 months
(49 years)
62 had gt50 relief or
significantly reduced pain
scores
SCS indikaacutecioacutek INeuropaacutethiaacutes (neurogeacuten) faacutejdalom
bull Perifeacuteriaacutes idegek seacuteruumlleacutese gyoumlkoumlk plexusok (idegrendszeri hiaacutenytuumlnet) seacuteruumlleacutes okai baleseti műteacutet pl lumbaacutelis discectomia (gyoumlk) nőgyoacutegyaacuteszati (inguinalis ideg) teacuterdműteacutetek (infrapatellaacuteris ideg) mastectomia (costo-brachiaacutelis ideg)
bull veacutegtag-amputaacutecioacute csonkfaacutejdalom jobban mint a fantom faacutejdalombull post-herpeses neuralgia amennyiben a bőreacuterzeacutes reacuteszlegesen megtartottbull post-irradiaacutecioacutes plexopaacutetiabull polyneuropaacutetiaacutek (diabeteses alkoholos) post-kemoteraacutepiaacutes (amennyiben a vastag rostok
műkoumldeacutese reacuteszlegesen megtartott)bull gerincvelő incomplett seacuteruumlleacutese -amennyiben a vastag eacuterzőrostok műkoumldeacutese megtartott eacutes a
segmentaacutelis faacutejdalom a seacuteruumlleacutes magassaacutegaacuteban leacutep felbull cervicaacutelis eacutes lumbosacralis radiculopaacutetiaacutek (compresszioacute ischaemia sebeacuteszi baleset
arachnoiditisbull CRPS II (causalga)bull DE bull plexus avulsioacute syringomyelia faacutejdalom nem csillapiacutethatoacutek bull nincs egyeteacuterteacutes a CRPS I (reflex sympaticus dystrophia)
SCS indikaacutecioacutek II
bull Kevert faacutejdalom szindroacutemaacutek
Falied back surgery syndroma = FBSS koraacutebbi gerincsebeacuteszeti beavatkozaacutes (postoperatiacutev fibrosis arachnoiditis)
Posztlaminektomiaacutes szindroacutemaangolszaacutesz failed back surgery szindroacutemaacutenak (FBSS)
bull faacutejdalom lokalizaacutecioacute alsoacute aacutegyeacuteki gerinc far
alsoacute veacutegtagok
bull etioloacutegia arachnoiditis epiduraacutelis heg
radiculitis mikro-instabilitaacutes rec
porckorongseacuterv gyulladaacutes
bull tapasztalatok alsoacute veacutegtagba terjedő
faacutejdalomra SCS hateacutekony
bull axiaacutelis faacutejdalmakra nem bizonyiacutetott
Incidencia FBSS
bull ranges 5 - 50
bull postdiscectomy 10-40
Etiologia FBSS
bull Scar tissue that forms around the surgery site interrupting normal neurological functioning
bull technicalities of the operation are not successful the performing surgeon had poor technique andor there is iatrogenic injury present
bull surgery is not performed at the site that causes the pain
bull surgery performed is not actually necessarybull patient is a poor fit for a successful surgerybull diagnosis was incorrectbull Complications of surgery arise
1 Anderson VC et al Current review of pain 20004105-11 5 Vaccaro AR et al Spine 200126 (24) S111-82 Leveque JC et al Neuromodulation 200141-9 6 Spengler DM et al Spine 19805356-603 Dario A et al Neuromodulation 20014105-110 7 Fager CA Freidberg SR Spine 1980587-944 Ohnmeiss DD et al The Spine Journal 2001358-363 8 Long DM Surgical management of pain 2002 354-64
FBSS okai eacutes tuumlnetei
bull FBSS cause1-7
ndash irreversible nerve injury
ndash surgical complications
ndash psychosocial problems
ndash inappropriate selection of patients for surgery
ndash recurrent herniation
ndash wrong level of operation
bull FBSS symptoms348
ndash lumbosacral postoperative fibrosis andor arachnoiditis
ndash root lesion
ndash dorsal compartment syndrome
ndash lateral spinal stenosis
SCS indikaacutecioacutek IIIAngina pectoris
bull New York Heart Association III-IV csoport (szignifikaacutens coronaacuteria stenosis egy vagy toumlbb szűkuumllet 70 )
bull myocardiaacutelis ischaemia reverzibilis angina gyoacutegyszeres revascularizaacutecioacutes beavatkozaacutesokkal nem enyhiacutethető
bull eacuteletminőseacuteguarr nitro-glicerin felhasznaacutelaacutesdarr anginaacutes rohamok szaacutemadarr jaacuteraacutestaacutevolsaacuteguarr
bull SCS anti-ischaemiaacutes hataacutes
bull nincs bizonyiacuteteacutek SCS hateacutekonysaacutegra instabil angina acut myocardiaacutelis infarctus vazospasticus angia maacutes sziacutevbetegseacuteg okozta anginaacutes faacutejdalmak csillapiacutetaacutesaacutera
Anginaacutes faacutejdalom
SCS tanulmaacutenyok hateacutekonysaacuteg I
bull Nienke (45 ) PT 1 eacutev koumlveteacutes eacuteletminőseacuteg szociaacutelis mentaacutelis fizikaacutelis teljesiacutetmeacuteny szignifikaacutensan javul
bull Hautvast (46) stabil angina pectorisban RT 6 heacutet koumlveteacutes
Randomizaacutelaacutes a stimulaacutetor OFF b csoport 3x1 oacuteranap ON vagy hirtelen anginaacuteban
anginaacutes rohamszaacutem csoumlkken
fizikai teljesiacutetőkeacutepesseacuteg javul
sublinguaacutelis nitraacutet felhasznaacutelaacutes csoumlkken
EKG-n az ischaemiaacutes epizoacutedusok csoumlkkennek
ST depresszioacute enyhuumll eacuteletminőseacuteg javul
anginaacutes faacutejdalom csoumlkken
SCS indikaacutecioacutek IIIAngina pectoris
bull tanulmaacutenyok eredmeacutenyei kedvezőek (39-43)
bull teraacutepiaacutes hataacutes hosszuacute taacutevuacute
bull nitraacutet bevitel csoumlkkenthető
bull faacutejdalomcsillapiacutetoacute hataacutesuacute
bull sziacutevizom veacuterkeringeacutes javul
bull PET tanulmaacuteny
ischaemiaacutes sziacutevizomban keringeacuteseacuteben
redistribucio alakul ki nyugalomban
eacutes gyoacutegyszer indukaacutelt stresszben(44)
SCS indikaacutecioacutek IVPerifeacuteriaacutes vasculaacuteris betegseacutegek
bull lassan progrediaacuteloacute perifeacuteriaacutes vasculaacuteris ischaemia -atherosclerosis (Fontaine 3 4 staacutedium )
bull vazospasticus betegseacuteg (pl Raynaud frostbite) gyoacutegyszeresen eacutersebeacuteszeti műteacutettel nem uralhatoacute veacutegtagfaacutejdalom
bull Buerger-koacuter
bull kontraindikaacutelt laacutebszaacuterfekeacutelygt 3 cm gangreacutena
SCS indikaacutecioacutek VCRPS
CRPS tuumlnetei
1 Harden RN et al Pain 199983211-219 6Birklein F et al Pain 19976949-54
2 Galer BS et al J Pain Symptom Manage 200020286-92 7 Schwartzman RJ Kerrigan J
Neurosurgery 19904057-61
3 Birklein F Handwerker HO Pain 2001 941-6 8 Zyluk A J Hand Surg 200126151-154
4 Rommel O et al Pain 19998095-101 9 Wasner G et al Neuro Clin
199816851-68
5 Thimineur M et al Clin J Pain 199814256-67
Sensory Motor dysfunctionIntense pain12 Weakness
Allodynia13 Decreased range of motion3
Hyperesthesia13 Tremor16
Hyperalgesia13 Dystonia7
Sensory deficits4 Myoclonus7
Decreased muscular strength8
Autonomic Dystrophic Swelling1 Increaseddecreased nailhair growth
Colourtemperature changes6 Skin changes (eg palor plantar fibrosis
Sweating abnormalities6 hyperkeratosis and thin glossy
skin9 )
Courtesy of Robert J Schwartzman MD
SCS indikaacutecioacutek VIAbdominaacutelis eacutes visceraacutelis faacutejdalom
szindroacutemaacutek
bull Faacutejdalom etioloacutegiaacuteja vaacuteltozatos
bull Ok gastrointestinaacutelis gastro-urinaacutelis
musculosceletaacutelis idegrendszeri
bull Megfigyeleacutes Th X myelotomia
daganatos pelvicus faacutejdalmat csillapiacutet
Mechanisms of SCS
bull Gate control theory
bull Direct inhibition of spinothalamic neurons
bull Descending modulatory effects
bull Alteration of sympathetic activity
bull Neurochemical modulation
GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Neurostimulaacutecioacute helye
bull perifeacuteriaacutes ideg PNS PNfS DRGS
bull gerincvelő SCS
bull meacutelyagyi DBS
bull motoros agykeacutereg MCS
Neurostimulaacutecioacutes faacutejdalomcsillapiacutetoacute műteacutetek indikaacutecioacutejaacutenak felaacutelliacutetaacutesa
bull faacutejdalom kezeleacuteseacuteben jaacuteratos szakemberek koumlzoumls doumlnteacutese
bull centrumokban (kivizsgaacutelaacutes kezeleacutes szoumlvődmeacutenyek elhaacuteriacutetaacutesa)
bull multidisciplinaacuteris (ideggyoacutegyaacutesz idegsebeacutesz psychiaacuteter psycholoacutegus anaesthesioloacutegus neuroradioloacutegus elektrofizioloacutegus mozgaacutesterapeuta) munkacsoport
Neurostimulaacutecioacute aacuteltalaacutenos kontraindikaacutecioacutek
(kroacutenikus faacutejdalom)
bull psychiaacutetriai koacuterkeacutepek (aktiacutev psychosis suacutelyos depresszioacute hipochondria szomatizaacutecioacutes betegseacutegek)
bull nem egyuumlttműkoumldő beteg
bull alkoholizmus kaacutebiacutetoacuteszer-eacutelvezet
bull suacutelyos kiacuteseacuterő betegseacuteg (coagulopathia immundeficiencia)
bull maacutes implantaacutelt pacemaker (pl sziacutev)
Neurostimulaacutecioacute műteacuteti szoumlvődmeacutenyek
bull korrigaacutelhatoacutek
bull implantaacutetummal (8-10) kapcsolatos
(elektroacuteda elmozdulaacutes seacuteruumlleacutes elektromos műkoumldeacutes zavar)
bull veacuterzeacutesek (1-5)
bull gyulladaacutesok (5-7)
Spinal cord stimulaacutecioacute (SCS)
bull Legneacutepszerűbb leggyakrabban alkalmazott
bull Első SCS daganatos faacutejdalom (Shealey 1967)
History of Spinal Cord StimulationShealy 1969
bull 1967 ndash Long and Wall PNS
bull 1969 ndash Shealy SCS in humans
bull 1975 ndash Dooley perc electrode
bull Mid 1970s ndash self-powered battery
bull 1980s - programmable quad electrode
bull 1980s -1990s ndash Primary cell IPG
bull 2004 ndash Rechargeable IPG
Clinical studies on SCS continue to support the effectiveness of this
therapy The following charts summarize studies of SCS and its
effects on the quality of life of patients
Reduction of Pain
ReferenceNumber of
PatientsFollow Up Results
Kumar17 410 8 years 74 had gt50 relief
North14 19 3 years 47 had gt50 relief
Barolat9 41 1 year50-65 had good to
excellent relief
Van Buyten18 123 3 years68 had good to excellent
relief
Cameron19 747Up to 59 months
(49 years)
62 had gt50 relief or
significantly reduced pain
scores
SCS indikaacutecioacutek INeuropaacutethiaacutes (neurogeacuten) faacutejdalom
bull Perifeacuteriaacutes idegek seacuteruumlleacutese gyoumlkoumlk plexusok (idegrendszeri hiaacutenytuumlnet) seacuteruumlleacutes okai baleseti műteacutet pl lumbaacutelis discectomia (gyoumlk) nőgyoacutegyaacuteszati (inguinalis ideg) teacuterdműteacutetek (infrapatellaacuteris ideg) mastectomia (costo-brachiaacutelis ideg)
bull veacutegtag-amputaacutecioacute csonkfaacutejdalom jobban mint a fantom faacutejdalombull post-herpeses neuralgia amennyiben a bőreacuterzeacutes reacuteszlegesen megtartottbull post-irradiaacutecioacutes plexopaacutetiabull polyneuropaacutetiaacutek (diabeteses alkoholos) post-kemoteraacutepiaacutes (amennyiben a vastag rostok
műkoumldeacutese reacuteszlegesen megtartott)bull gerincvelő incomplett seacuteruumlleacutese -amennyiben a vastag eacuterzőrostok műkoumldeacutese megtartott eacutes a
segmentaacutelis faacutejdalom a seacuteruumlleacutes magassaacutegaacuteban leacutep felbull cervicaacutelis eacutes lumbosacralis radiculopaacutetiaacutek (compresszioacute ischaemia sebeacuteszi baleset
arachnoiditisbull CRPS II (causalga)bull DE bull plexus avulsioacute syringomyelia faacutejdalom nem csillapiacutethatoacutek bull nincs egyeteacuterteacutes a CRPS I (reflex sympaticus dystrophia)
SCS indikaacutecioacutek II
bull Kevert faacutejdalom szindroacutemaacutek
Falied back surgery syndroma = FBSS koraacutebbi gerincsebeacuteszeti beavatkozaacutes (postoperatiacutev fibrosis arachnoiditis)
Posztlaminektomiaacutes szindroacutemaangolszaacutesz failed back surgery szindroacutemaacutenak (FBSS)
bull faacutejdalom lokalizaacutecioacute alsoacute aacutegyeacuteki gerinc far
alsoacute veacutegtagok
bull etioloacutegia arachnoiditis epiduraacutelis heg
radiculitis mikro-instabilitaacutes rec
porckorongseacuterv gyulladaacutes
bull tapasztalatok alsoacute veacutegtagba terjedő
faacutejdalomra SCS hateacutekony
bull axiaacutelis faacutejdalmakra nem bizonyiacutetott
Incidencia FBSS
bull ranges 5 - 50
bull postdiscectomy 10-40
Etiologia FBSS
bull Scar tissue that forms around the surgery site interrupting normal neurological functioning
bull technicalities of the operation are not successful the performing surgeon had poor technique andor there is iatrogenic injury present
bull surgery is not performed at the site that causes the pain
bull surgery performed is not actually necessarybull patient is a poor fit for a successful surgerybull diagnosis was incorrectbull Complications of surgery arise
1 Anderson VC et al Current review of pain 20004105-11 5 Vaccaro AR et al Spine 200126 (24) S111-82 Leveque JC et al Neuromodulation 200141-9 6 Spengler DM et al Spine 19805356-603 Dario A et al Neuromodulation 20014105-110 7 Fager CA Freidberg SR Spine 1980587-944 Ohnmeiss DD et al The Spine Journal 2001358-363 8 Long DM Surgical management of pain 2002 354-64
FBSS okai eacutes tuumlnetei
bull FBSS cause1-7
ndash irreversible nerve injury
ndash surgical complications
ndash psychosocial problems
ndash inappropriate selection of patients for surgery
ndash recurrent herniation
ndash wrong level of operation
bull FBSS symptoms348
ndash lumbosacral postoperative fibrosis andor arachnoiditis
ndash root lesion
ndash dorsal compartment syndrome
ndash lateral spinal stenosis
SCS indikaacutecioacutek IIIAngina pectoris
bull New York Heart Association III-IV csoport (szignifikaacutens coronaacuteria stenosis egy vagy toumlbb szűkuumllet 70 )
bull myocardiaacutelis ischaemia reverzibilis angina gyoacutegyszeres revascularizaacutecioacutes beavatkozaacutesokkal nem enyhiacutethető
bull eacuteletminőseacuteguarr nitro-glicerin felhasznaacutelaacutesdarr anginaacutes rohamok szaacutemadarr jaacuteraacutestaacutevolsaacuteguarr
bull SCS anti-ischaemiaacutes hataacutes
bull nincs bizonyiacuteteacutek SCS hateacutekonysaacutegra instabil angina acut myocardiaacutelis infarctus vazospasticus angia maacutes sziacutevbetegseacuteg okozta anginaacutes faacutejdalmak csillapiacutetaacutesaacutera
Anginaacutes faacutejdalom
SCS tanulmaacutenyok hateacutekonysaacuteg I
bull Nienke (45 ) PT 1 eacutev koumlveteacutes eacuteletminőseacuteg szociaacutelis mentaacutelis fizikaacutelis teljesiacutetmeacuteny szignifikaacutensan javul
bull Hautvast (46) stabil angina pectorisban RT 6 heacutet koumlveteacutes
Randomizaacutelaacutes a stimulaacutetor OFF b csoport 3x1 oacuteranap ON vagy hirtelen anginaacuteban
anginaacutes rohamszaacutem csoumlkken
fizikai teljesiacutetőkeacutepesseacuteg javul
sublinguaacutelis nitraacutet felhasznaacutelaacutes csoumlkken
EKG-n az ischaemiaacutes epizoacutedusok csoumlkkennek
ST depresszioacute enyhuumll eacuteletminőseacuteg javul
anginaacutes faacutejdalom csoumlkken
SCS indikaacutecioacutek IIIAngina pectoris
bull tanulmaacutenyok eredmeacutenyei kedvezőek (39-43)
bull teraacutepiaacutes hataacutes hosszuacute taacutevuacute
bull nitraacutet bevitel csoumlkkenthető
bull faacutejdalomcsillapiacutetoacute hataacutesuacute
bull sziacutevizom veacuterkeringeacutes javul
bull PET tanulmaacuteny
ischaemiaacutes sziacutevizomban keringeacuteseacuteben
redistribucio alakul ki nyugalomban
eacutes gyoacutegyszer indukaacutelt stresszben(44)
SCS indikaacutecioacutek IVPerifeacuteriaacutes vasculaacuteris betegseacutegek
bull lassan progrediaacuteloacute perifeacuteriaacutes vasculaacuteris ischaemia -atherosclerosis (Fontaine 3 4 staacutedium )
bull vazospasticus betegseacuteg (pl Raynaud frostbite) gyoacutegyszeresen eacutersebeacuteszeti műteacutettel nem uralhatoacute veacutegtagfaacutejdalom
bull Buerger-koacuter
bull kontraindikaacutelt laacutebszaacuterfekeacutelygt 3 cm gangreacutena
SCS indikaacutecioacutek VCRPS
CRPS tuumlnetei
1 Harden RN et al Pain 199983211-219 6Birklein F et al Pain 19976949-54
2 Galer BS et al J Pain Symptom Manage 200020286-92 7 Schwartzman RJ Kerrigan J
Neurosurgery 19904057-61
3 Birklein F Handwerker HO Pain 2001 941-6 8 Zyluk A J Hand Surg 200126151-154
4 Rommel O et al Pain 19998095-101 9 Wasner G et al Neuro Clin
199816851-68
5 Thimineur M et al Clin J Pain 199814256-67
Sensory Motor dysfunctionIntense pain12 Weakness
Allodynia13 Decreased range of motion3
Hyperesthesia13 Tremor16
Hyperalgesia13 Dystonia7
Sensory deficits4 Myoclonus7
Decreased muscular strength8
Autonomic Dystrophic Swelling1 Increaseddecreased nailhair growth
Colourtemperature changes6 Skin changes (eg palor plantar fibrosis
Sweating abnormalities6 hyperkeratosis and thin glossy
skin9 )
Courtesy of Robert J Schwartzman MD
SCS indikaacutecioacutek VIAbdominaacutelis eacutes visceraacutelis faacutejdalom
szindroacutemaacutek
bull Faacutejdalom etioloacutegiaacuteja vaacuteltozatos
bull Ok gastrointestinaacutelis gastro-urinaacutelis
musculosceletaacutelis idegrendszeri
bull Megfigyeleacutes Th X myelotomia
daganatos pelvicus faacutejdalmat csillapiacutet
Mechanisms of SCS
bull Gate control theory
bull Direct inhibition of spinothalamic neurons
bull Descending modulatory effects
bull Alteration of sympathetic activity
bull Neurochemical modulation
GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Neurostimulaacutecioacutes faacutejdalomcsillapiacutetoacute műteacutetek indikaacutecioacutejaacutenak felaacutelliacutetaacutesa
bull faacutejdalom kezeleacuteseacuteben jaacuteratos szakemberek koumlzoumls doumlnteacutese
bull centrumokban (kivizsgaacutelaacutes kezeleacutes szoumlvődmeacutenyek elhaacuteriacutetaacutesa)
bull multidisciplinaacuteris (ideggyoacutegyaacutesz idegsebeacutesz psychiaacuteter psycholoacutegus anaesthesioloacutegus neuroradioloacutegus elektrofizioloacutegus mozgaacutesterapeuta) munkacsoport
Neurostimulaacutecioacute aacuteltalaacutenos kontraindikaacutecioacutek
(kroacutenikus faacutejdalom)
bull psychiaacutetriai koacuterkeacutepek (aktiacutev psychosis suacutelyos depresszioacute hipochondria szomatizaacutecioacutes betegseacutegek)
bull nem egyuumlttműkoumldő beteg
bull alkoholizmus kaacutebiacutetoacuteszer-eacutelvezet
bull suacutelyos kiacuteseacuterő betegseacuteg (coagulopathia immundeficiencia)
bull maacutes implantaacutelt pacemaker (pl sziacutev)
Neurostimulaacutecioacute műteacuteti szoumlvődmeacutenyek
bull korrigaacutelhatoacutek
bull implantaacutetummal (8-10) kapcsolatos
(elektroacuteda elmozdulaacutes seacuteruumlleacutes elektromos műkoumldeacutes zavar)
bull veacuterzeacutesek (1-5)
bull gyulladaacutesok (5-7)
Spinal cord stimulaacutecioacute (SCS)
bull Legneacutepszerűbb leggyakrabban alkalmazott
bull Első SCS daganatos faacutejdalom (Shealey 1967)
History of Spinal Cord StimulationShealy 1969
bull 1967 ndash Long and Wall PNS
bull 1969 ndash Shealy SCS in humans
bull 1975 ndash Dooley perc electrode
bull Mid 1970s ndash self-powered battery
bull 1980s - programmable quad electrode
bull 1980s -1990s ndash Primary cell IPG
bull 2004 ndash Rechargeable IPG
Clinical studies on SCS continue to support the effectiveness of this
therapy The following charts summarize studies of SCS and its
effects on the quality of life of patients
Reduction of Pain
ReferenceNumber of
PatientsFollow Up Results
Kumar17 410 8 years 74 had gt50 relief
North14 19 3 years 47 had gt50 relief
Barolat9 41 1 year50-65 had good to
excellent relief
Van Buyten18 123 3 years68 had good to excellent
relief
Cameron19 747Up to 59 months
(49 years)
62 had gt50 relief or
significantly reduced pain
scores
SCS indikaacutecioacutek INeuropaacutethiaacutes (neurogeacuten) faacutejdalom
bull Perifeacuteriaacutes idegek seacuteruumlleacutese gyoumlkoumlk plexusok (idegrendszeri hiaacutenytuumlnet) seacuteruumlleacutes okai baleseti műteacutet pl lumbaacutelis discectomia (gyoumlk) nőgyoacutegyaacuteszati (inguinalis ideg) teacuterdműteacutetek (infrapatellaacuteris ideg) mastectomia (costo-brachiaacutelis ideg)
bull veacutegtag-amputaacutecioacute csonkfaacutejdalom jobban mint a fantom faacutejdalombull post-herpeses neuralgia amennyiben a bőreacuterzeacutes reacuteszlegesen megtartottbull post-irradiaacutecioacutes plexopaacutetiabull polyneuropaacutetiaacutek (diabeteses alkoholos) post-kemoteraacutepiaacutes (amennyiben a vastag rostok
műkoumldeacutese reacuteszlegesen megtartott)bull gerincvelő incomplett seacuteruumlleacutese -amennyiben a vastag eacuterzőrostok műkoumldeacutese megtartott eacutes a
segmentaacutelis faacutejdalom a seacuteruumlleacutes magassaacutegaacuteban leacutep felbull cervicaacutelis eacutes lumbosacralis radiculopaacutetiaacutek (compresszioacute ischaemia sebeacuteszi baleset
arachnoiditisbull CRPS II (causalga)bull DE bull plexus avulsioacute syringomyelia faacutejdalom nem csillapiacutethatoacutek bull nincs egyeteacuterteacutes a CRPS I (reflex sympaticus dystrophia)
SCS indikaacutecioacutek II
bull Kevert faacutejdalom szindroacutemaacutek
Falied back surgery syndroma = FBSS koraacutebbi gerincsebeacuteszeti beavatkozaacutes (postoperatiacutev fibrosis arachnoiditis)
Posztlaminektomiaacutes szindroacutemaangolszaacutesz failed back surgery szindroacutemaacutenak (FBSS)
bull faacutejdalom lokalizaacutecioacute alsoacute aacutegyeacuteki gerinc far
alsoacute veacutegtagok
bull etioloacutegia arachnoiditis epiduraacutelis heg
radiculitis mikro-instabilitaacutes rec
porckorongseacuterv gyulladaacutes
bull tapasztalatok alsoacute veacutegtagba terjedő
faacutejdalomra SCS hateacutekony
bull axiaacutelis faacutejdalmakra nem bizonyiacutetott
Incidencia FBSS
bull ranges 5 - 50
bull postdiscectomy 10-40
Etiologia FBSS
bull Scar tissue that forms around the surgery site interrupting normal neurological functioning
bull technicalities of the operation are not successful the performing surgeon had poor technique andor there is iatrogenic injury present
bull surgery is not performed at the site that causes the pain
bull surgery performed is not actually necessarybull patient is a poor fit for a successful surgerybull diagnosis was incorrectbull Complications of surgery arise
1 Anderson VC et al Current review of pain 20004105-11 5 Vaccaro AR et al Spine 200126 (24) S111-82 Leveque JC et al Neuromodulation 200141-9 6 Spengler DM et al Spine 19805356-603 Dario A et al Neuromodulation 20014105-110 7 Fager CA Freidberg SR Spine 1980587-944 Ohnmeiss DD et al The Spine Journal 2001358-363 8 Long DM Surgical management of pain 2002 354-64
FBSS okai eacutes tuumlnetei
bull FBSS cause1-7
ndash irreversible nerve injury
ndash surgical complications
ndash psychosocial problems
ndash inappropriate selection of patients for surgery
ndash recurrent herniation
ndash wrong level of operation
bull FBSS symptoms348
ndash lumbosacral postoperative fibrosis andor arachnoiditis
ndash root lesion
ndash dorsal compartment syndrome
ndash lateral spinal stenosis
SCS indikaacutecioacutek IIIAngina pectoris
bull New York Heart Association III-IV csoport (szignifikaacutens coronaacuteria stenosis egy vagy toumlbb szűkuumllet 70 )
bull myocardiaacutelis ischaemia reverzibilis angina gyoacutegyszeres revascularizaacutecioacutes beavatkozaacutesokkal nem enyhiacutethető
bull eacuteletminőseacuteguarr nitro-glicerin felhasznaacutelaacutesdarr anginaacutes rohamok szaacutemadarr jaacuteraacutestaacutevolsaacuteguarr
bull SCS anti-ischaemiaacutes hataacutes
bull nincs bizonyiacuteteacutek SCS hateacutekonysaacutegra instabil angina acut myocardiaacutelis infarctus vazospasticus angia maacutes sziacutevbetegseacuteg okozta anginaacutes faacutejdalmak csillapiacutetaacutesaacutera
Anginaacutes faacutejdalom
SCS tanulmaacutenyok hateacutekonysaacuteg I
bull Nienke (45 ) PT 1 eacutev koumlveteacutes eacuteletminőseacuteg szociaacutelis mentaacutelis fizikaacutelis teljesiacutetmeacuteny szignifikaacutensan javul
bull Hautvast (46) stabil angina pectorisban RT 6 heacutet koumlveteacutes
Randomizaacutelaacutes a stimulaacutetor OFF b csoport 3x1 oacuteranap ON vagy hirtelen anginaacuteban
anginaacutes rohamszaacutem csoumlkken
fizikai teljesiacutetőkeacutepesseacuteg javul
sublinguaacutelis nitraacutet felhasznaacutelaacutes csoumlkken
EKG-n az ischaemiaacutes epizoacutedusok csoumlkkennek
ST depresszioacute enyhuumll eacuteletminőseacuteg javul
anginaacutes faacutejdalom csoumlkken
SCS indikaacutecioacutek IIIAngina pectoris
bull tanulmaacutenyok eredmeacutenyei kedvezőek (39-43)
bull teraacutepiaacutes hataacutes hosszuacute taacutevuacute
bull nitraacutet bevitel csoumlkkenthető
bull faacutejdalomcsillapiacutetoacute hataacutesuacute
bull sziacutevizom veacuterkeringeacutes javul
bull PET tanulmaacuteny
ischaemiaacutes sziacutevizomban keringeacuteseacuteben
redistribucio alakul ki nyugalomban
eacutes gyoacutegyszer indukaacutelt stresszben(44)
SCS indikaacutecioacutek IVPerifeacuteriaacutes vasculaacuteris betegseacutegek
bull lassan progrediaacuteloacute perifeacuteriaacutes vasculaacuteris ischaemia -atherosclerosis (Fontaine 3 4 staacutedium )
bull vazospasticus betegseacuteg (pl Raynaud frostbite) gyoacutegyszeresen eacutersebeacuteszeti műteacutettel nem uralhatoacute veacutegtagfaacutejdalom
bull Buerger-koacuter
bull kontraindikaacutelt laacutebszaacuterfekeacutelygt 3 cm gangreacutena
SCS indikaacutecioacutek VCRPS
CRPS tuumlnetei
1 Harden RN et al Pain 199983211-219 6Birklein F et al Pain 19976949-54
2 Galer BS et al J Pain Symptom Manage 200020286-92 7 Schwartzman RJ Kerrigan J
Neurosurgery 19904057-61
3 Birklein F Handwerker HO Pain 2001 941-6 8 Zyluk A J Hand Surg 200126151-154
4 Rommel O et al Pain 19998095-101 9 Wasner G et al Neuro Clin
199816851-68
5 Thimineur M et al Clin J Pain 199814256-67
Sensory Motor dysfunctionIntense pain12 Weakness
Allodynia13 Decreased range of motion3
Hyperesthesia13 Tremor16
Hyperalgesia13 Dystonia7
Sensory deficits4 Myoclonus7
Decreased muscular strength8
Autonomic Dystrophic Swelling1 Increaseddecreased nailhair growth
Colourtemperature changes6 Skin changes (eg palor plantar fibrosis
Sweating abnormalities6 hyperkeratosis and thin glossy
skin9 )
Courtesy of Robert J Schwartzman MD
SCS indikaacutecioacutek VIAbdominaacutelis eacutes visceraacutelis faacutejdalom
szindroacutemaacutek
bull Faacutejdalom etioloacutegiaacuteja vaacuteltozatos
bull Ok gastrointestinaacutelis gastro-urinaacutelis
musculosceletaacutelis idegrendszeri
bull Megfigyeleacutes Th X myelotomia
daganatos pelvicus faacutejdalmat csillapiacutet
Mechanisms of SCS
bull Gate control theory
bull Direct inhibition of spinothalamic neurons
bull Descending modulatory effects
bull Alteration of sympathetic activity
bull Neurochemical modulation
GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Neurostimulaacutecioacute aacuteltalaacutenos kontraindikaacutecioacutek
(kroacutenikus faacutejdalom)
bull psychiaacutetriai koacuterkeacutepek (aktiacutev psychosis suacutelyos depresszioacute hipochondria szomatizaacutecioacutes betegseacutegek)
bull nem egyuumlttműkoumldő beteg
bull alkoholizmus kaacutebiacutetoacuteszer-eacutelvezet
bull suacutelyos kiacuteseacuterő betegseacuteg (coagulopathia immundeficiencia)
bull maacutes implantaacutelt pacemaker (pl sziacutev)
Neurostimulaacutecioacute műteacuteti szoumlvődmeacutenyek
bull korrigaacutelhatoacutek
bull implantaacutetummal (8-10) kapcsolatos
(elektroacuteda elmozdulaacutes seacuteruumlleacutes elektromos műkoumldeacutes zavar)
bull veacuterzeacutesek (1-5)
bull gyulladaacutesok (5-7)
Spinal cord stimulaacutecioacute (SCS)
bull Legneacutepszerűbb leggyakrabban alkalmazott
bull Első SCS daganatos faacutejdalom (Shealey 1967)
History of Spinal Cord StimulationShealy 1969
bull 1967 ndash Long and Wall PNS
bull 1969 ndash Shealy SCS in humans
bull 1975 ndash Dooley perc electrode
bull Mid 1970s ndash self-powered battery
bull 1980s - programmable quad electrode
bull 1980s -1990s ndash Primary cell IPG
bull 2004 ndash Rechargeable IPG
Clinical studies on SCS continue to support the effectiveness of this
therapy The following charts summarize studies of SCS and its
effects on the quality of life of patients
Reduction of Pain
ReferenceNumber of
PatientsFollow Up Results
Kumar17 410 8 years 74 had gt50 relief
North14 19 3 years 47 had gt50 relief
Barolat9 41 1 year50-65 had good to
excellent relief
Van Buyten18 123 3 years68 had good to excellent
relief
Cameron19 747Up to 59 months
(49 years)
62 had gt50 relief or
significantly reduced pain
scores
SCS indikaacutecioacutek INeuropaacutethiaacutes (neurogeacuten) faacutejdalom
bull Perifeacuteriaacutes idegek seacuteruumlleacutese gyoumlkoumlk plexusok (idegrendszeri hiaacutenytuumlnet) seacuteruumlleacutes okai baleseti műteacutet pl lumbaacutelis discectomia (gyoumlk) nőgyoacutegyaacuteszati (inguinalis ideg) teacuterdműteacutetek (infrapatellaacuteris ideg) mastectomia (costo-brachiaacutelis ideg)
bull veacutegtag-amputaacutecioacute csonkfaacutejdalom jobban mint a fantom faacutejdalombull post-herpeses neuralgia amennyiben a bőreacuterzeacutes reacuteszlegesen megtartottbull post-irradiaacutecioacutes plexopaacutetiabull polyneuropaacutetiaacutek (diabeteses alkoholos) post-kemoteraacutepiaacutes (amennyiben a vastag rostok
műkoumldeacutese reacuteszlegesen megtartott)bull gerincvelő incomplett seacuteruumlleacutese -amennyiben a vastag eacuterzőrostok műkoumldeacutese megtartott eacutes a
segmentaacutelis faacutejdalom a seacuteruumlleacutes magassaacutegaacuteban leacutep felbull cervicaacutelis eacutes lumbosacralis radiculopaacutetiaacutek (compresszioacute ischaemia sebeacuteszi baleset
arachnoiditisbull CRPS II (causalga)bull DE bull plexus avulsioacute syringomyelia faacutejdalom nem csillapiacutethatoacutek bull nincs egyeteacuterteacutes a CRPS I (reflex sympaticus dystrophia)
SCS indikaacutecioacutek II
bull Kevert faacutejdalom szindroacutemaacutek
Falied back surgery syndroma = FBSS koraacutebbi gerincsebeacuteszeti beavatkozaacutes (postoperatiacutev fibrosis arachnoiditis)
Posztlaminektomiaacutes szindroacutemaangolszaacutesz failed back surgery szindroacutemaacutenak (FBSS)
bull faacutejdalom lokalizaacutecioacute alsoacute aacutegyeacuteki gerinc far
alsoacute veacutegtagok
bull etioloacutegia arachnoiditis epiduraacutelis heg
radiculitis mikro-instabilitaacutes rec
porckorongseacuterv gyulladaacutes
bull tapasztalatok alsoacute veacutegtagba terjedő
faacutejdalomra SCS hateacutekony
bull axiaacutelis faacutejdalmakra nem bizonyiacutetott
Incidencia FBSS
bull ranges 5 - 50
bull postdiscectomy 10-40
Etiologia FBSS
bull Scar tissue that forms around the surgery site interrupting normal neurological functioning
bull technicalities of the operation are not successful the performing surgeon had poor technique andor there is iatrogenic injury present
bull surgery is not performed at the site that causes the pain
bull surgery performed is not actually necessarybull patient is a poor fit for a successful surgerybull diagnosis was incorrectbull Complications of surgery arise
1 Anderson VC et al Current review of pain 20004105-11 5 Vaccaro AR et al Spine 200126 (24) S111-82 Leveque JC et al Neuromodulation 200141-9 6 Spengler DM et al Spine 19805356-603 Dario A et al Neuromodulation 20014105-110 7 Fager CA Freidberg SR Spine 1980587-944 Ohnmeiss DD et al The Spine Journal 2001358-363 8 Long DM Surgical management of pain 2002 354-64
FBSS okai eacutes tuumlnetei
bull FBSS cause1-7
ndash irreversible nerve injury
ndash surgical complications
ndash psychosocial problems
ndash inappropriate selection of patients for surgery
ndash recurrent herniation
ndash wrong level of operation
bull FBSS symptoms348
ndash lumbosacral postoperative fibrosis andor arachnoiditis
ndash root lesion
ndash dorsal compartment syndrome
ndash lateral spinal stenosis
SCS indikaacutecioacutek IIIAngina pectoris
bull New York Heart Association III-IV csoport (szignifikaacutens coronaacuteria stenosis egy vagy toumlbb szűkuumllet 70 )
bull myocardiaacutelis ischaemia reverzibilis angina gyoacutegyszeres revascularizaacutecioacutes beavatkozaacutesokkal nem enyhiacutethető
bull eacuteletminőseacuteguarr nitro-glicerin felhasznaacutelaacutesdarr anginaacutes rohamok szaacutemadarr jaacuteraacutestaacutevolsaacuteguarr
bull SCS anti-ischaemiaacutes hataacutes
bull nincs bizonyiacuteteacutek SCS hateacutekonysaacutegra instabil angina acut myocardiaacutelis infarctus vazospasticus angia maacutes sziacutevbetegseacuteg okozta anginaacutes faacutejdalmak csillapiacutetaacutesaacutera
Anginaacutes faacutejdalom
SCS tanulmaacutenyok hateacutekonysaacuteg I
bull Nienke (45 ) PT 1 eacutev koumlveteacutes eacuteletminőseacuteg szociaacutelis mentaacutelis fizikaacutelis teljesiacutetmeacuteny szignifikaacutensan javul
bull Hautvast (46) stabil angina pectorisban RT 6 heacutet koumlveteacutes
Randomizaacutelaacutes a stimulaacutetor OFF b csoport 3x1 oacuteranap ON vagy hirtelen anginaacuteban
anginaacutes rohamszaacutem csoumlkken
fizikai teljesiacutetőkeacutepesseacuteg javul
sublinguaacutelis nitraacutet felhasznaacutelaacutes csoumlkken
EKG-n az ischaemiaacutes epizoacutedusok csoumlkkennek
ST depresszioacute enyhuumll eacuteletminőseacuteg javul
anginaacutes faacutejdalom csoumlkken
SCS indikaacutecioacutek IIIAngina pectoris
bull tanulmaacutenyok eredmeacutenyei kedvezőek (39-43)
bull teraacutepiaacutes hataacutes hosszuacute taacutevuacute
bull nitraacutet bevitel csoumlkkenthető
bull faacutejdalomcsillapiacutetoacute hataacutesuacute
bull sziacutevizom veacuterkeringeacutes javul
bull PET tanulmaacuteny
ischaemiaacutes sziacutevizomban keringeacuteseacuteben
redistribucio alakul ki nyugalomban
eacutes gyoacutegyszer indukaacutelt stresszben(44)
SCS indikaacutecioacutek IVPerifeacuteriaacutes vasculaacuteris betegseacutegek
bull lassan progrediaacuteloacute perifeacuteriaacutes vasculaacuteris ischaemia -atherosclerosis (Fontaine 3 4 staacutedium )
bull vazospasticus betegseacuteg (pl Raynaud frostbite) gyoacutegyszeresen eacutersebeacuteszeti műteacutettel nem uralhatoacute veacutegtagfaacutejdalom
bull Buerger-koacuter
bull kontraindikaacutelt laacutebszaacuterfekeacutelygt 3 cm gangreacutena
SCS indikaacutecioacutek VCRPS
CRPS tuumlnetei
1 Harden RN et al Pain 199983211-219 6Birklein F et al Pain 19976949-54
2 Galer BS et al J Pain Symptom Manage 200020286-92 7 Schwartzman RJ Kerrigan J
Neurosurgery 19904057-61
3 Birklein F Handwerker HO Pain 2001 941-6 8 Zyluk A J Hand Surg 200126151-154
4 Rommel O et al Pain 19998095-101 9 Wasner G et al Neuro Clin
199816851-68
5 Thimineur M et al Clin J Pain 199814256-67
Sensory Motor dysfunctionIntense pain12 Weakness
Allodynia13 Decreased range of motion3
Hyperesthesia13 Tremor16
Hyperalgesia13 Dystonia7
Sensory deficits4 Myoclonus7
Decreased muscular strength8
Autonomic Dystrophic Swelling1 Increaseddecreased nailhair growth
Colourtemperature changes6 Skin changes (eg palor plantar fibrosis
Sweating abnormalities6 hyperkeratosis and thin glossy
skin9 )
Courtesy of Robert J Schwartzman MD
SCS indikaacutecioacutek VIAbdominaacutelis eacutes visceraacutelis faacutejdalom
szindroacutemaacutek
bull Faacutejdalom etioloacutegiaacuteja vaacuteltozatos
bull Ok gastrointestinaacutelis gastro-urinaacutelis
musculosceletaacutelis idegrendszeri
bull Megfigyeleacutes Th X myelotomia
daganatos pelvicus faacutejdalmat csillapiacutet
Mechanisms of SCS
bull Gate control theory
bull Direct inhibition of spinothalamic neurons
bull Descending modulatory effects
bull Alteration of sympathetic activity
bull Neurochemical modulation
GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Neurostimulaacutecioacute műteacuteti szoumlvődmeacutenyek
bull korrigaacutelhatoacutek
bull implantaacutetummal (8-10) kapcsolatos
(elektroacuteda elmozdulaacutes seacuteruumlleacutes elektromos műkoumldeacutes zavar)
bull veacuterzeacutesek (1-5)
bull gyulladaacutesok (5-7)
Spinal cord stimulaacutecioacute (SCS)
bull Legneacutepszerűbb leggyakrabban alkalmazott
bull Első SCS daganatos faacutejdalom (Shealey 1967)
History of Spinal Cord StimulationShealy 1969
bull 1967 ndash Long and Wall PNS
bull 1969 ndash Shealy SCS in humans
bull 1975 ndash Dooley perc electrode
bull Mid 1970s ndash self-powered battery
bull 1980s - programmable quad electrode
bull 1980s -1990s ndash Primary cell IPG
bull 2004 ndash Rechargeable IPG
Clinical studies on SCS continue to support the effectiveness of this
therapy The following charts summarize studies of SCS and its
effects on the quality of life of patients
Reduction of Pain
ReferenceNumber of
PatientsFollow Up Results
Kumar17 410 8 years 74 had gt50 relief
North14 19 3 years 47 had gt50 relief
Barolat9 41 1 year50-65 had good to
excellent relief
Van Buyten18 123 3 years68 had good to excellent
relief
Cameron19 747Up to 59 months
(49 years)
62 had gt50 relief or
significantly reduced pain
scores
SCS indikaacutecioacutek INeuropaacutethiaacutes (neurogeacuten) faacutejdalom
bull Perifeacuteriaacutes idegek seacuteruumlleacutese gyoumlkoumlk plexusok (idegrendszeri hiaacutenytuumlnet) seacuteruumlleacutes okai baleseti műteacutet pl lumbaacutelis discectomia (gyoumlk) nőgyoacutegyaacuteszati (inguinalis ideg) teacuterdműteacutetek (infrapatellaacuteris ideg) mastectomia (costo-brachiaacutelis ideg)
bull veacutegtag-amputaacutecioacute csonkfaacutejdalom jobban mint a fantom faacutejdalombull post-herpeses neuralgia amennyiben a bőreacuterzeacutes reacuteszlegesen megtartottbull post-irradiaacutecioacutes plexopaacutetiabull polyneuropaacutetiaacutek (diabeteses alkoholos) post-kemoteraacutepiaacutes (amennyiben a vastag rostok
műkoumldeacutese reacuteszlegesen megtartott)bull gerincvelő incomplett seacuteruumlleacutese -amennyiben a vastag eacuterzőrostok műkoumldeacutese megtartott eacutes a
segmentaacutelis faacutejdalom a seacuteruumlleacutes magassaacutegaacuteban leacutep felbull cervicaacutelis eacutes lumbosacralis radiculopaacutetiaacutek (compresszioacute ischaemia sebeacuteszi baleset
arachnoiditisbull CRPS II (causalga)bull DE bull plexus avulsioacute syringomyelia faacutejdalom nem csillapiacutethatoacutek bull nincs egyeteacuterteacutes a CRPS I (reflex sympaticus dystrophia)
SCS indikaacutecioacutek II
bull Kevert faacutejdalom szindroacutemaacutek
Falied back surgery syndroma = FBSS koraacutebbi gerincsebeacuteszeti beavatkozaacutes (postoperatiacutev fibrosis arachnoiditis)
Posztlaminektomiaacutes szindroacutemaangolszaacutesz failed back surgery szindroacutemaacutenak (FBSS)
bull faacutejdalom lokalizaacutecioacute alsoacute aacutegyeacuteki gerinc far
alsoacute veacutegtagok
bull etioloacutegia arachnoiditis epiduraacutelis heg
radiculitis mikro-instabilitaacutes rec
porckorongseacuterv gyulladaacutes
bull tapasztalatok alsoacute veacutegtagba terjedő
faacutejdalomra SCS hateacutekony
bull axiaacutelis faacutejdalmakra nem bizonyiacutetott
Incidencia FBSS
bull ranges 5 - 50
bull postdiscectomy 10-40
Etiologia FBSS
bull Scar tissue that forms around the surgery site interrupting normal neurological functioning
bull technicalities of the operation are not successful the performing surgeon had poor technique andor there is iatrogenic injury present
bull surgery is not performed at the site that causes the pain
bull surgery performed is not actually necessarybull patient is a poor fit for a successful surgerybull diagnosis was incorrectbull Complications of surgery arise
1 Anderson VC et al Current review of pain 20004105-11 5 Vaccaro AR et al Spine 200126 (24) S111-82 Leveque JC et al Neuromodulation 200141-9 6 Spengler DM et al Spine 19805356-603 Dario A et al Neuromodulation 20014105-110 7 Fager CA Freidberg SR Spine 1980587-944 Ohnmeiss DD et al The Spine Journal 2001358-363 8 Long DM Surgical management of pain 2002 354-64
FBSS okai eacutes tuumlnetei
bull FBSS cause1-7
ndash irreversible nerve injury
ndash surgical complications
ndash psychosocial problems
ndash inappropriate selection of patients for surgery
ndash recurrent herniation
ndash wrong level of operation
bull FBSS symptoms348
ndash lumbosacral postoperative fibrosis andor arachnoiditis
ndash root lesion
ndash dorsal compartment syndrome
ndash lateral spinal stenosis
SCS indikaacutecioacutek IIIAngina pectoris
bull New York Heart Association III-IV csoport (szignifikaacutens coronaacuteria stenosis egy vagy toumlbb szűkuumllet 70 )
bull myocardiaacutelis ischaemia reverzibilis angina gyoacutegyszeres revascularizaacutecioacutes beavatkozaacutesokkal nem enyhiacutethető
bull eacuteletminőseacuteguarr nitro-glicerin felhasznaacutelaacutesdarr anginaacutes rohamok szaacutemadarr jaacuteraacutestaacutevolsaacuteguarr
bull SCS anti-ischaemiaacutes hataacutes
bull nincs bizonyiacuteteacutek SCS hateacutekonysaacutegra instabil angina acut myocardiaacutelis infarctus vazospasticus angia maacutes sziacutevbetegseacuteg okozta anginaacutes faacutejdalmak csillapiacutetaacutesaacutera
Anginaacutes faacutejdalom
SCS tanulmaacutenyok hateacutekonysaacuteg I
bull Nienke (45 ) PT 1 eacutev koumlveteacutes eacuteletminőseacuteg szociaacutelis mentaacutelis fizikaacutelis teljesiacutetmeacuteny szignifikaacutensan javul
bull Hautvast (46) stabil angina pectorisban RT 6 heacutet koumlveteacutes
Randomizaacutelaacutes a stimulaacutetor OFF b csoport 3x1 oacuteranap ON vagy hirtelen anginaacuteban
anginaacutes rohamszaacutem csoumlkken
fizikai teljesiacutetőkeacutepesseacuteg javul
sublinguaacutelis nitraacutet felhasznaacutelaacutes csoumlkken
EKG-n az ischaemiaacutes epizoacutedusok csoumlkkennek
ST depresszioacute enyhuumll eacuteletminőseacuteg javul
anginaacutes faacutejdalom csoumlkken
SCS indikaacutecioacutek IIIAngina pectoris
bull tanulmaacutenyok eredmeacutenyei kedvezőek (39-43)
bull teraacutepiaacutes hataacutes hosszuacute taacutevuacute
bull nitraacutet bevitel csoumlkkenthető
bull faacutejdalomcsillapiacutetoacute hataacutesuacute
bull sziacutevizom veacuterkeringeacutes javul
bull PET tanulmaacuteny
ischaemiaacutes sziacutevizomban keringeacuteseacuteben
redistribucio alakul ki nyugalomban
eacutes gyoacutegyszer indukaacutelt stresszben(44)
SCS indikaacutecioacutek IVPerifeacuteriaacutes vasculaacuteris betegseacutegek
bull lassan progrediaacuteloacute perifeacuteriaacutes vasculaacuteris ischaemia -atherosclerosis (Fontaine 3 4 staacutedium )
bull vazospasticus betegseacuteg (pl Raynaud frostbite) gyoacutegyszeresen eacutersebeacuteszeti műteacutettel nem uralhatoacute veacutegtagfaacutejdalom
bull Buerger-koacuter
bull kontraindikaacutelt laacutebszaacuterfekeacutelygt 3 cm gangreacutena
SCS indikaacutecioacutek VCRPS
CRPS tuumlnetei
1 Harden RN et al Pain 199983211-219 6Birklein F et al Pain 19976949-54
2 Galer BS et al J Pain Symptom Manage 200020286-92 7 Schwartzman RJ Kerrigan J
Neurosurgery 19904057-61
3 Birklein F Handwerker HO Pain 2001 941-6 8 Zyluk A J Hand Surg 200126151-154
4 Rommel O et al Pain 19998095-101 9 Wasner G et al Neuro Clin
199816851-68
5 Thimineur M et al Clin J Pain 199814256-67
Sensory Motor dysfunctionIntense pain12 Weakness
Allodynia13 Decreased range of motion3
Hyperesthesia13 Tremor16
Hyperalgesia13 Dystonia7
Sensory deficits4 Myoclonus7
Decreased muscular strength8
Autonomic Dystrophic Swelling1 Increaseddecreased nailhair growth
Colourtemperature changes6 Skin changes (eg palor plantar fibrosis
Sweating abnormalities6 hyperkeratosis and thin glossy
skin9 )
Courtesy of Robert J Schwartzman MD
SCS indikaacutecioacutek VIAbdominaacutelis eacutes visceraacutelis faacutejdalom
szindroacutemaacutek
bull Faacutejdalom etioloacutegiaacuteja vaacuteltozatos
bull Ok gastrointestinaacutelis gastro-urinaacutelis
musculosceletaacutelis idegrendszeri
bull Megfigyeleacutes Th X myelotomia
daganatos pelvicus faacutejdalmat csillapiacutet
Mechanisms of SCS
bull Gate control theory
bull Direct inhibition of spinothalamic neurons
bull Descending modulatory effects
bull Alteration of sympathetic activity
bull Neurochemical modulation
GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Spinal cord stimulaacutecioacute (SCS)
bull Legneacutepszerűbb leggyakrabban alkalmazott
bull Első SCS daganatos faacutejdalom (Shealey 1967)
History of Spinal Cord StimulationShealy 1969
bull 1967 ndash Long and Wall PNS
bull 1969 ndash Shealy SCS in humans
bull 1975 ndash Dooley perc electrode
bull Mid 1970s ndash self-powered battery
bull 1980s - programmable quad electrode
bull 1980s -1990s ndash Primary cell IPG
bull 2004 ndash Rechargeable IPG
Clinical studies on SCS continue to support the effectiveness of this
therapy The following charts summarize studies of SCS and its
effects on the quality of life of patients
Reduction of Pain
ReferenceNumber of
PatientsFollow Up Results
Kumar17 410 8 years 74 had gt50 relief
North14 19 3 years 47 had gt50 relief
Barolat9 41 1 year50-65 had good to
excellent relief
Van Buyten18 123 3 years68 had good to excellent
relief
Cameron19 747Up to 59 months
(49 years)
62 had gt50 relief or
significantly reduced pain
scores
SCS indikaacutecioacutek INeuropaacutethiaacutes (neurogeacuten) faacutejdalom
bull Perifeacuteriaacutes idegek seacuteruumlleacutese gyoumlkoumlk plexusok (idegrendszeri hiaacutenytuumlnet) seacuteruumlleacutes okai baleseti műteacutet pl lumbaacutelis discectomia (gyoumlk) nőgyoacutegyaacuteszati (inguinalis ideg) teacuterdműteacutetek (infrapatellaacuteris ideg) mastectomia (costo-brachiaacutelis ideg)
bull veacutegtag-amputaacutecioacute csonkfaacutejdalom jobban mint a fantom faacutejdalombull post-herpeses neuralgia amennyiben a bőreacuterzeacutes reacuteszlegesen megtartottbull post-irradiaacutecioacutes plexopaacutetiabull polyneuropaacutetiaacutek (diabeteses alkoholos) post-kemoteraacutepiaacutes (amennyiben a vastag rostok
műkoumldeacutese reacuteszlegesen megtartott)bull gerincvelő incomplett seacuteruumlleacutese -amennyiben a vastag eacuterzőrostok műkoumldeacutese megtartott eacutes a
segmentaacutelis faacutejdalom a seacuteruumlleacutes magassaacutegaacuteban leacutep felbull cervicaacutelis eacutes lumbosacralis radiculopaacutetiaacutek (compresszioacute ischaemia sebeacuteszi baleset
arachnoiditisbull CRPS II (causalga)bull DE bull plexus avulsioacute syringomyelia faacutejdalom nem csillapiacutethatoacutek bull nincs egyeteacuterteacutes a CRPS I (reflex sympaticus dystrophia)
SCS indikaacutecioacutek II
bull Kevert faacutejdalom szindroacutemaacutek
Falied back surgery syndroma = FBSS koraacutebbi gerincsebeacuteszeti beavatkozaacutes (postoperatiacutev fibrosis arachnoiditis)
Posztlaminektomiaacutes szindroacutemaangolszaacutesz failed back surgery szindroacutemaacutenak (FBSS)
bull faacutejdalom lokalizaacutecioacute alsoacute aacutegyeacuteki gerinc far
alsoacute veacutegtagok
bull etioloacutegia arachnoiditis epiduraacutelis heg
radiculitis mikro-instabilitaacutes rec
porckorongseacuterv gyulladaacutes
bull tapasztalatok alsoacute veacutegtagba terjedő
faacutejdalomra SCS hateacutekony
bull axiaacutelis faacutejdalmakra nem bizonyiacutetott
Incidencia FBSS
bull ranges 5 - 50
bull postdiscectomy 10-40
Etiologia FBSS
bull Scar tissue that forms around the surgery site interrupting normal neurological functioning
bull technicalities of the operation are not successful the performing surgeon had poor technique andor there is iatrogenic injury present
bull surgery is not performed at the site that causes the pain
bull surgery performed is not actually necessarybull patient is a poor fit for a successful surgerybull diagnosis was incorrectbull Complications of surgery arise
1 Anderson VC et al Current review of pain 20004105-11 5 Vaccaro AR et al Spine 200126 (24) S111-82 Leveque JC et al Neuromodulation 200141-9 6 Spengler DM et al Spine 19805356-603 Dario A et al Neuromodulation 20014105-110 7 Fager CA Freidberg SR Spine 1980587-944 Ohnmeiss DD et al The Spine Journal 2001358-363 8 Long DM Surgical management of pain 2002 354-64
FBSS okai eacutes tuumlnetei
bull FBSS cause1-7
ndash irreversible nerve injury
ndash surgical complications
ndash psychosocial problems
ndash inappropriate selection of patients for surgery
ndash recurrent herniation
ndash wrong level of operation
bull FBSS symptoms348
ndash lumbosacral postoperative fibrosis andor arachnoiditis
ndash root lesion
ndash dorsal compartment syndrome
ndash lateral spinal stenosis
SCS indikaacutecioacutek IIIAngina pectoris
bull New York Heart Association III-IV csoport (szignifikaacutens coronaacuteria stenosis egy vagy toumlbb szűkuumllet 70 )
bull myocardiaacutelis ischaemia reverzibilis angina gyoacutegyszeres revascularizaacutecioacutes beavatkozaacutesokkal nem enyhiacutethető
bull eacuteletminőseacuteguarr nitro-glicerin felhasznaacutelaacutesdarr anginaacutes rohamok szaacutemadarr jaacuteraacutestaacutevolsaacuteguarr
bull SCS anti-ischaemiaacutes hataacutes
bull nincs bizonyiacuteteacutek SCS hateacutekonysaacutegra instabil angina acut myocardiaacutelis infarctus vazospasticus angia maacutes sziacutevbetegseacuteg okozta anginaacutes faacutejdalmak csillapiacutetaacutesaacutera
Anginaacutes faacutejdalom
SCS tanulmaacutenyok hateacutekonysaacuteg I
bull Nienke (45 ) PT 1 eacutev koumlveteacutes eacuteletminőseacuteg szociaacutelis mentaacutelis fizikaacutelis teljesiacutetmeacuteny szignifikaacutensan javul
bull Hautvast (46) stabil angina pectorisban RT 6 heacutet koumlveteacutes
Randomizaacutelaacutes a stimulaacutetor OFF b csoport 3x1 oacuteranap ON vagy hirtelen anginaacuteban
anginaacutes rohamszaacutem csoumlkken
fizikai teljesiacutetőkeacutepesseacuteg javul
sublinguaacutelis nitraacutet felhasznaacutelaacutes csoumlkken
EKG-n az ischaemiaacutes epizoacutedusok csoumlkkennek
ST depresszioacute enyhuumll eacuteletminőseacuteg javul
anginaacutes faacutejdalom csoumlkken
SCS indikaacutecioacutek IIIAngina pectoris
bull tanulmaacutenyok eredmeacutenyei kedvezőek (39-43)
bull teraacutepiaacutes hataacutes hosszuacute taacutevuacute
bull nitraacutet bevitel csoumlkkenthető
bull faacutejdalomcsillapiacutetoacute hataacutesuacute
bull sziacutevizom veacuterkeringeacutes javul
bull PET tanulmaacuteny
ischaemiaacutes sziacutevizomban keringeacuteseacuteben
redistribucio alakul ki nyugalomban
eacutes gyoacutegyszer indukaacutelt stresszben(44)
SCS indikaacutecioacutek IVPerifeacuteriaacutes vasculaacuteris betegseacutegek
bull lassan progrediaacuteloacute perifeacuteriaacutes vasculaacuteris ischaemia -atherosclerosis (Fontaine 3 4 staacutedium )
bull vazospasticus betegseacuteg (pl Raynaud frostbite) gyoacutegyszeresen eacutersebeacuteszeti műteacutettel nem uralhatoacute veacutegtagfaacutejdalom
bull Buerger-koacuter
bull kontraindikaacutelt laacutebszaacuterfekeacutelygt 3 cm gangreacutena
SCS indikaacutecioacutek VCRPS
CRPS tuumlnetei
1 Harden RN et al Pain 199983211-219 6Birklein F et al Pain 19976949-54
2 Galer BS et al J Pain Symptom Manage 200020286-92 7 Schwartzman RJ Kerrigan J
Neurosurgery 19904057-61
3 Birklein F Handwerker HO Pain 2001 941-6 8 Zyluk A J Hand Surg 200126151-154
4 Rommel O et al Pain 19998095-101 9 Wasner G et al Neuro Clin
199816851-68
5 Thimineur M et al Clin J Pain 199814256-67
Sensory Motor dysfunctionIntense pain12 Weakness
Allodynia13 Decreased range of motion3
Hyperesthesia13 Tremor16
Hyperalgesia13 Dystonia7
Sensory deficits4 Myoclonus7
Decreased muscular strength8
Autonomic Dystrophic Swelling1 Increaseddecreased nailhair growth
Colourtemperature changes6 Skin changes (eg palor plantar fibrosis
Sweating abnormalities6 hyperkeratosis and thin glossy
skin9 )
Courtesy of Robert J Schwartzman MD
SCS indikaacutecioacutek VIAbdominaacutelis eacutes visceraacutelis faacutejdalom
szindroacutemaacutek
bull Faacutejdalom etioloacutegiaacuteja vaacuteltozatos
bull Ok gastrointestinaacutelis gastro-urinaacutelis
musculosceletaacutelis idegrendszeri
bull Megfigyeleacutes Th X myelotomia
daganatos pelvicus faacutejdalmat csillapiacutet
Mechanisms of SCS
bull Gate control theory
bull Direct inhibition of spinothalamic neurons
bull Descending modulatory effects
bull Alteration of sympathetic activity
bull Neurochemical modulation
GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

History of Spinal Cord StimulationShealy 1969
bull 1967 ndash Long and Wall PNS
bull 1969 ndash Shealy SCS in humans
bull 1975 ndash Dooley perc electrode
bull Mid 1970s ndash self-powered battery
bull 1980s - programmable quad electrode
bull 1980s -1990s ndash Primary cell IPG
bull 2004 ndash Rechargeable IPG
Clinical studies on SCS continue to support the effectiveness of this
therapy The following charts summarize studies of SCS and its
effects on the quality of life of patients
Reduction of Pain
ReferenceNumber of
PatientsFollow Up Results
Kumar17 410 8 years 74 had gt50 relief
North14 19 3 years 47 had gt50 relief
Barolat9 41 1 year50-65 had good to
excellent relief
Van Buyten18 123 3 years68 had good to excellent
relief
Cameron19 747Up to 59 months
(49 years)
62 had gt50 relief or
significantly reduced pain
scores
SCS indikaacutecioacutek INeuropaacutethiaacutes (neurogeacuten) faacutejdalom
bull Perifeacuteriaacutes idegek seacuteruumlleacutese gyoumlkoumlk plexusok (idegrendszeri hiaacutenytuumlnet) seacuteruumlleacutes okai baleseti műteacutet pl lumbaacutelis discectomia (gyoumlk) nőgyoacutegyaacuteszati (inguinalis ideg) teacuterdműteacutetek (infrapatellaacuteris ideg) mastectomia (costo-brachiaacutelis ideg)
bull veacutegtag-amputaacutecioacute csonkfaacutejdalom jobban mint a fantom faacutejdalombull post-herpeses neuralgia amennyiben a bőreacuterzeacutes reacuteszlegesen megtartottbull post-irradiaacutecioacutes plexopaacutetiabull polyneuropaacutetiaacutek (diabeteses alkoholos) post-kemoteraacutepiaacutes (amennyiben a vastag rostok
műkoumldeacutese reacuteszlegesen megtartott)bull gerincvelő incomplett seacuteruumlleacutese -amennyiben a vastag eacuterzőrostok műkoumldeacutese megtartott eacutes a
segmentaacutelis faacutejdalom a seacuteruumlleacutes magassaacutegaacuteban leacutep felbull cervicaacutelis eacutes lumbosacralis radiculopaacutetiaacutek (compresszioacute ischaemia sebeacuteszi baleset
arachnoiditisbull CRPS II (causalga)bull DE bull plexus avulsioacute syringomyelia faacutejdalom nem csillapiacutethatoacutek bull nincs egyeteacuterteacutes a CRPS I (reflex sympaticus dystrophia)
SCS indikaacutecioacutek II
bull Kevert faacutejdalom szindroacutemaacutek
Falied back surgery syndroma = FBSS koraacutebbi gerincsebeacuteszeti beavatkozaacutes (postoperatiacutev fibrosis arachnoiditis)
Posztlaminektomiaacutes szindroacutemaangolszaacutesz failed back surgery szindroacutemaacutenak (FBSS)
bull faacutejdalom lokalizaacutecioacute alsoacute aacutegyeacuteki gerinc far
alsoacute veacutegtagok
bull etioloacutegia arachnoiditis epiduraacutelis heg
radiculitis mikro-instabilitaacutes rec
porckorongseacuterv gyulladaacutes
bull tapasztalatok alsoacute veacutegtagba terjedő
faacutejdalomra SCS hateacutekony
bull axiaacutelis faacutejdalmakra nem bizonyiacutetott
Incidencia FBSS
bull ranges 5 - 50
bull postdiscectomy 10-40
Etiologia FBSS
bull Scar tissue that forms around the surgery site interrupting normal neurological functioning
bull technicalities of the operation are not successful the performing surgeon had poor technique andor there is iatrogenic injury present
bull surgery is not performed at the site that causes the pain
bull surgery performed is not actually necessarybull patient is a poor fit for a successful surgerybull diagnosis was incorrectbull Complications of surgery arise
1 Anderson VC et al Current review of pain 20004105-11 5 Vaccaro AR et al Spine 200126 (24) S111-82 Leveque JC et al Neuromodulation 200141-9 6 Spengler DM et al Spine 19805356-603 Dario A et al Neuromodulation 20014105-110 7 Fager CA Freidberg SR Spine 1980587-944 Ohnmeiss DD et al The Spine Journal 2001358-363 8 Long DM Surgical management of pain 2002 354-64
FBSS okai eacutes tuumlnetei
bull FBSS cause1-7
ndash irreversible nerve injury
ndash surgical complications
ndash psychosocial problems
ndash inappropriate selection of patients for surgery
ndash recurrent herniation
ndash wrong level of operation
bull FBSS symptoms348
ndash lumbosacral postoperative fibrosis andor arachnoiditis
ndash root lesion
ndash dorsal compartment syndrome
ndash lateral spinal stenosis
SCS indikaacutecioacutek IIIAngina pectoris
bull New York Heart Association III-IV csoport (szignifikaacutens coronaacuteria stenosis egy vagy toumlbb szűkuumllet 70 )
bull myocardiaacutelis ischaemia reverzibilis angina gyoacutegyszeres revascularizaacutecioacutes beavatkozaacutesokkal nem enyhiacutethető
bull eacuteletminőseacuteguarr nitro-glicerin felhasznaacutelaacutesdarr anginaacutes rohamok szaacutemadarr jaacuteraacutestaacutevolsaacuteguarr
bull SCS anti-ischaemiaacutes hataacutes
bull nincs bizonyiacuteteacutek SCS hateacutekonysaacutegra instabil angina acut myocardiaacutelis infarctus vazospasticus angia maacutes sziacutevbetegseacuteg okozta anginaacutes faacutejdalmak csillapiacutetaacutesaacutera
Anginaacutes faacutejdalom
SCS tanulmaacutenyok hateacutekonysaacuteg I
bull Nienke (45 ) PT 1 eacutev koumlveteacutes eacuteletminőseacuteg szociaacutelis mentaacutelis fizikaacutelis teljesiacutetmeacuteny szignifikaacutensan javul
bull Hautvast (46) stabil angina pectorisban RT 6 heacutet koumlveteacutes
Randomizaacutelaacutes a stimulaacutetor OFF b csoport 3x1 oacuteranap ON vagy hirtelen anginaacuteban
anginaacutes rohamszaacutem csoumlkken
fizikai teljesiacutetőkeacutepesseacuteg javul
sublinguaacutelis nitraacutet felhasznaacutelaacutes csoumlkken
EKG-n az ischaemiaacutes epizoacutedusok csoumlkkennek
ST depresszioacute enyhuumll eacuteletminőseacuteg javul
anginaacutes faacutejdalom csoumlkken
SCS indikaacutecioacutek IIIAngina pectoris
bull tanulmaacutenyok eredmeacutenyei kedvezőek (39-43)
bull teraacutepiaacutes hataacutes hosszuacute taacutevuacute
bull nitraacutet bevitel csoumlkkenthető
bull faacutejdalomcsillapiacutetoacute hataacutesuacute
bull sziacutevizom veacuterkeringeacutes javul
bull PET tanulmaacuteny
ischaemiaacutes sziacutevizomban keringeacuteseacuteben
redistribucio alakul ki nyugalomban
eacutes gyoacutegyszer indukaacutelt stresszben(44)
SCS indikaacutecioacutek IVPerifeacuteriaacutes vasculaacuteris betegseacutegek
bull lassan progrediaacuteloacute perifeacuteriaacutes vasculaacuteris ischaemia -atherosclerosis (Fontaine 3 4 staacutedium )
bull vazospasticus betegseacuteg (pl Raynaud frostbite) gyoacutegyszeresen eacutersebeacuteszeti műteacutettel nem uralhatoacute veacutegtagfaacutejdalom
bull Buerger-koacuter
bull kontraindikaacutelt laacutebszaacuterfekeacutelygt 3 cm gangreacutena
SCS indikaacutecioacutek VCRPS
CRPS tuumlnetei
1 Harden RN et al Pain 199983211-219 6Birklein F et al Pain 19976949-54
2 Galer BS et al J Pain Symptom Manage 200020286-92 7 Schwartzman RJ Kerrigan J
Neurosurgery 19904057-61
3 Birklein F Handwerker HO Pain 2001 941-6 8 Zyluk A J Hand Surg 200126151-154
4 Rommel O et al Pain 19998095-101 9 Wasner G et al Neuro Clin
199816851-68
5 Thimineur M et al Clin J Pain 199814256-67
Sensory Motor dysfunctionIntense pain12 Weakness
Allodynia13 Decreased range of motion3
Hyperesthesia13 Tremor16
Hyperalgesia13 Dystonia7
Sensory deficits4 Myoclonus7
Decreased muscular strength8
Autonomic Dystrophic Swelling1 Increaseddecreased nailhair growth
Colourtemperature changes6 Skin changes (eg palor plantar fibrosis
Sweating abnormalities6 hyperkeratosis and thin glossy
skin9 )
Courtesy of Robert J Schwartzman MD
SCS indikaacutecioacutek VIAbdominaacutelis eacutes visceraacutelis faacutejdalom
szindroacutemaacutek
bull Faacutejdalom etioloacutegiaacuteja vaacuteltozatos
bull Ok gastrointestinaacutelis gastro-urinaacutelis
musculosceletaacutelis idegrendszeri
bull Megfigyeleacutes Th X myelotomia
daganatos pelvicus faacutejdalmat csillapiacutet
Mechanisms of SCS
bull Gate control theory
bull Direct inhibition of spinothalamic neurons
bull Descending modulatory effects
bull Alteration of sympathetic activity
bull Neurochemical modulation
GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Clinical studies on SCS continue to support the effectiveness of this
therapy The following charts summarize studies of SCS and its
effects on the quality of life of patients
Reduction of Pain
ReferenceNumber of
PatientsFollow Up Results
Kumar17 410 8 years 74 had gt50 relief
North14 19 3 years 47 had gt50 relief
Barolat9 41 1 year50-65 had good to
excellent relief
Van Buyten18 123 3 years68 had good to excellent
relief
Cameron19 747Up to 59 months
(49 years)
62 had gt50 relief or
significantly reduced pain
scores
SCS indikaacutecioacutek INeuropaacutethiaacutes (neurogeacuten) faacutejdalom
bull Perifeacuteriaacutes idegek seacuteruumlleacutese gyoumlkoumlk plexusok (idegrendszeri hiaacutenytuumlnet) seacuteruumlleacutes okai baleseti műteacutet pl lumbaacutelis discectomia (gyoumlk) nőgyoacutegyaacuteszati (inguinalis ideg) teacuterdműteacutetek (infrapatellaacuteris ideg) mastectomia (costo-brachiaacutelis ideg)
bull veacutegtag-amputaacutecioacute csonkfaacutejdalom jobban mint a fantom faacutejdalombull post-herpeses neuralgia amennyiben a bőreacuterzeacutes reacuteszlegesen megtartottbull post-irradiaacutecioacutes plexopaacutetiabull polyneuropaacutetiaacutek (diabeteses alkoholos) post-kemoteraacutepiaacutes (amennyiben a vastag rostok
műkoumldeacutese reacuteszlegesen megtartott)bull gerincvelő incomplett seacuteruumlleacutese -amennyiben a vastag eacuterzőrostok műkoumldeacutese megtartott eacutes a
segmentaacutelis faacutejdalom a seacuteruumlleacutes magassaacutegaacuteban leacutep felbull cervicaacutelis eacutes lumbosacralis radiculopaacutetiaacutek (compresszioacute ischaemia sebeacuteszi baleset
arachnoiditisbull CRPS II (causalga)bull DE bull plexus avulsioacute syringomyelia faacutejdalom nem csillapiacutethatoacutek bull nincs egyeteacuterteacutes a CRPS I (reflex sympaticus dystrophia)
SCS indikaacutecioacutek II
bull Kevert faacutejdalom szindroacutemaacutek
Falied back surgery syndroma = FBSS koraacutebbi gerincsebeacuteszeti beavatkozaacutes (postoperatiacutev fibrosis arachnoiditis)
Posztlaminektomiaacutes szindroacutemaangolszaacutesz failed back surgery szindroacutemaacutenak (FBSS)
bull faacutejdalom lokalizaacutecioacute alsoacute aacutegyeacuteki gerinc far
alsoacute veacutegtagok
bull etioloacutegia arachnoiditis epiduraacutelis heg
radiculitis mikro-instabilitaacutes rec
porckorongseacuterv gyulladaacutes
bull tapasztalatok alsoacute veacutegtagba terjedő
faacutejdalomra SCS hateacutekony
bull axiaacutelis faacutejdalmakra nem bizonyiacutetott
Incidencia FBSS
bull ranges 5 - 50
bull postdiscectomy 10-40
Etiologia FBSS
bull Scar tissue that forms around the surgery site interrupting normal neurological functioning
bull technicalities of the operation are not successful the performing surgeon had poor technique andor there is iatrogenic injury present
bull surgery is not performed at the site that causes the pain
bull surgery performed is not actually necessarybull patient is a poor fit for a successful surgerybull diagnosis was incorrectbull Complications of surgery arise
1 Anderson VC et al Current review of pain 20004105-11 5 Vaccaro AR et al Spine 200126 (24) S111-82 Leveque JC et al Neuromodulation 200141-9 6 Spengler DM et al Spine 19805356-603 Dario A et al Neuromodulation 20014105-110 7 Fager CA Freidberg SR Spine 1980587-944 Ohnmeiss DD et al The Spine Journal 2001358-363 8 Long DM Surgical management of pain 2002 354-64
FBSS okai eacutes tuumlnetei
bull FBSS cause1-7
ndash irreversible nerve injury
ndash surgical complications
ndash psychosocial problems
ndash inappropriate selection of patients for surgery
ndash recurrent herniation
ndash wrong level of operation
bull FBSS symptoms348
ndash lumbosacral postoperative fibrosis andor arachnoiditis
ndash root lesion
ndash dorsal compartment syndrome
ndash lateral spinal stenosis
SCS indikaacutecioacutek IIIAngina pectoris
bull New York Heart Association III-IV csoport (szignifikaacutens coronaacuteria stenosis egy vagy toumlbb szűkuumllet 70 )
bull myocardiaacutelis ischaemia reverzibilis angina gyoacutegyszeres revascularizaacutecioacutes beavatkozaacutesokkal nem enyhiacutethető
bull eacuteletminőseacuteguarr nitro-glicerin felhasznaacutelaacutesdarr anginaacutes rohamok szaacutemadarr jaacuteraacutestaacutevolsaacuteguarr
bull SCS anti-ischaemiaacutes hataacutes
bull nincs bizonyiacuteteacutek SCS hateacutekonysaacutegra instabil angina acut myocardiaacutelis infarctus vazospasticus angia maacutes sziacutevbetegseacuteg okozta anginaacutes faacutejdalmak csillapiacutetaacutesaacutera
Anginaacutes faacutejdalom
SCS tanulmaacutenyok hateacutekonysaacuteg I
bull Nienke (45 ) PT 1 eacutev koumlveteacutes eacuteletminőseacuteg szociaacutelis mentaacutelis fizikaacutelis teljesiacutetmeacuteny szignifikaacutensan javul
bull Hautvast (46) stabil angina pectorisban RT 6 heacutet koumlveteacutes
Randomizaacutelaacutes a stimulaacutetor OFF b csoport 3x1 oacuteranap ON vagy hirtelen anginaacuteban
anginaacutes rohamszaacutem csoumlkken
fizikai teljesiacutetőkeacutepesseacuteg javul
sublinguaacutelis nitraacutet felhasznaacutelaacutes csoumlkken
EKG-n az ischaemiaacutes epizoacutedusok csoumlkkennek
ST depresszioacute enyhuumll eacuteletminőseacuteg javul
anginaacutes faacutejdalom csoumlkken
SCS indikaacutecioacutek IIIAngina pectoris
bull tanulmaacutenyok eredmeacutenyei kedvezőek (39-43)
bull teraacutepiaacutes hataacutes hosszuacute taacutevuacute
bull nitraacutet bevitel csoumlkkenthető
bull faacutejdalomcsillapiacutetoacute hataacutesuacute
bull sziacutevizom veacuterkeringeacutes javul
bull PET tanulmaacuteny
ischaemiaacutes sziacutevizomban keringeacuteseacuteben
redistribucio alakul ki nyugalomban
eacutes gyoacutegyszer indukaacutelt stresszben(44)
SCS indikaacutecioacutek IVPerifeacuteriaacutes vasculaacuteris betegseacutegek
bull lassan progrediaacuteloacute perifeacuteriaacutes vasculaacuteris ischaemia -atherosclerosis (Fontaine 3 4 staacutedium )
bull vazospasticus betegseacuteg (pl Raynaud frostbite) gyoacutegyszeresen eacutersebeacuteszeti műteacutettel nem uralhatoacute veacutegtagfaacutejdalom
bull Buerger-koacuter
bull kontraindikaacutelt laacutebszaacuterfekeacutelygt 3 cm gangreacutena
SCS indikaacutecioacutek VCRPS
CRPS tuumlnetei
1 Harden RN et al Pain 199983211-219 6Birklein F et al Pain 19976949-54
2 Galer BS et al J Pain Symptom Manage 200020286-92 7 Schwartzman RJ Kerrigan J
Neurosurgery 19904057-61
3 Birklein F Handwerker HO Pain 2001 941-6 8 Zyluk A J Hand Surg 200126151-154
4 Rommel O et al Pain 19998095-101 9 Wasner G et al Neuro Clin
199816851-68
5 Thimineur M et al Clin J Pain 199814256-67
Sensory Motor dysfunctionIntense pain12 Weakness
Allodynia13 Decreased range of motion3
Hyperesthesia13 Tremor16
Hyperalgesia13 Dystonia7
Sensory deficits4 Myoclonus7
Decreased muscular strength8
Autonomic Dystrophic Swelling1 Increaseddecreased nailhair growth
Colourtemperature changes6 Skin changes (eg palor plantar fibrosis
Sweating abnormalities6 hyperkeratosis and thin glossy
skin9 )
Courtesy of Robert J Schwartzman MD
SCS indikaacutecioacutek VIAbdominaacutelis eacutes visceraacutelis faacutejdalom
szindroacutemaacutek
bull Faacutejdalom etioloacutegiaacuteja vaacuteltozatos
bull Ok gastrointestinaacutelis gastro-urinaacutelis
musculosceletaacutelis idegrendszeri
bull Megfigyeleacutes Th X myelotomia
daganatos pelvicus faacutejdalmat csillapiacutet
Mechanisms of SCS
bull Gate control theory
bull Direct inhibition of spinothalamic neurons
bull Descending modulatory effects
bull Alteration of sympathetic activity
bull Neurochemical modulation
GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

SCS indikaacutecioacutek INeuropaacutethiaacutes (neurogeacuten) faacutejdalom
bull Perifeacuteriaacutes idegek seacuteruumlleacutese gyoumlkoumlk plexusok (idegrendszeri hiaacutenytuumlnet) seacuteruumlleacutes okai baleseti műteacutet pl lumbaacutelis discectomia (gyoumlk) nőgyoacutegyaacuteszati (inguinalis ideg) teacuterdműteacutetek (infrapatellaacuteris ideg) mastectomia (costo-brachiaacutelis ideg)
bull veacutegtag-amputaacutecioacute csonkfaacutejdalom jobban mint a fantom faacutejdalombull post-herpeses neuralgia amennyiben a bőreacuterzeacutes reacuteszlegesen megtartottbull post-irradiaacutecioacutes plexopaacutetiabull polyneuropaacutetiaacutek (diabeteses alkoholos) post-kemoteraacutepiaacutes (amennyiben a vastag rostok
műkoumldeacutese reacuteszlegesen megtartott)bull gerincvelő incomplett seacuteruumlleacutese -amennyiben a vastag eacuterzőrostok műkoumldeacutese megtartott eacutes a
segmentaacutelis faacutejdalom a seacuteruumlleacutes magassaacutegaacuteban leacutep felbull cervicaacutelis eacutes lumbosacralis radiculopaacutetiaacutek (compresszioacute ischaemia sebeacuteszi baleset
arachnoiditisbull CRPS II (causalga)bull DE bull plexus avulsioacute syringomyelia faacutejdalom nem csillapiacutethatoacutek bull nincs egyeteacuterteacutes a CRPS I (reflex sympaticus dystrophia)
SCS indikaacutecioacutek II
bull Kevert faacutejdalom szindroacutemaacutek
Falied back surgery syndroma = FBSS koraacutebbi gerincsebeacuteszeti beavatkozaacutes (postoperatiacutev fibrosis arachnoiditis)
Posztlaminektomiaacutes szindroacutemaangolszaacutesz failed back surgery szindroacutemaacutenak (FBSS)
bull faacutejdalom lokalizaacutecioacute alsoacute aacutegyeacuteki gerinc far
alsoacute veacutegtagok
bull etioloacutegia arachnoiditis epiduraacutelis heg
radiculitis mikro-instabilitaacutes rec
porckorongseacuterv gyulladaacutes
bull tapasztalatok alsoacute veacutegtagba terjedő
faacutejdalomra SCS hateacutekony
bull axiaacutelis faacutejdalmakra nem bizonyiacutetott
Incidencia FBSS
bull ranges 5 - 50
bull postdiscectomy 10-40
Etiologia FBSS
bull Scar tissue that forms around the surgery site interrupting normal neurological functioning
bull technicalities of the operation are not successful the performing surgeon had poor technique andor there is iatrogenic injury present
bull surgery is not performed at the site that causes the pain
bull surgery performed is not actually necessarybull patient is a poor fit for a successful surgerybull diagnosis was incorrectbull Complications of surgery arise
1 Anderson VC et al Current review of pain 20004105-11 5 Vaccaro AR et al Spine 200126 (24) S111-82 Leveque JC et al Neuromodulation 200141-9 6 Spengler DM et al Spine 19805356-603 Dario A et al Neuromodulation 20014105-110 7 Fager CA Freidberg SR Spine 1980587-944 Ohnmeiss DD et al The Spine Journal 2001358-363 8 Long DM Surgical management of pain 2002 354-64
FBSS okai eacutes tuumlnetei
bull FBSS cause1-7
ndash irreversible nerve injury
ndash surgical complications
ndash psychosocial problems
ndash inappropriate selection of patients for surgery
ndash recurrent herniation
ndash wrong level of operation
bull FBSS symptoms348
ndash lumbosacral postoperative fibrosis andor arachnoiditis
ndash root lesion
ndash dorsal compartment syndrome
ndash lateral spinal stenosis
SCS indikaacutecioacutek IIIAngina pectoris
bull New York Heart Association III-IV csoport (szignifikaacutens coronaacuteria stenosis egy vagy toumlbb szűkuumllet 70 )
bull myocardiaacutelis ischaemia reverzibilis angina gyoacutegyszeres revascularizaacutecioacutes beavatkozaacutesokkal nem enyhiacutethető
bull eacuteletminőseacuteguarr nitro-glicerin felhasznaacutelaacutesdarr anginaacutes rohamok szaacutemadarr jaacuteraacutestaacutevolsaacuteguarr
bull SCS anti-ischaemiaacutes hataacutes
bull nincs bizonyiacuteteacutek SCS hateacutekonysaacutegra instabil angina acut myocardiaacutelis infarctus vazospasticus angia maacutes sziacutevbetegseacuteg okozta anginaacutes faacutejdalmak csillapiacutetaacutesaacutera
Anginaacutes faacutejdalom
SCS tanulmaacutenyok hateacutekonysaacuteg I
bull Nienke (45 ) PT 1 eacutev koumlveteacutes eacuteletminőseacuteg szociaacutelis mentaacutelis fizikaacutelis teljesiacutetmeacuteny szignifikaacutensan javul
bull Hautvast (46) stabil angina pectorisban RT 6 heacutet koumlveteacutes
Randomizaacutelaacutes a stimulaacutetor OFF b csoport 3x1 oacuteranap ON vagy hirtelen anginaacuteban
anginaacutes rohamszaacutem csoumlkken
fizikai teljesiacutetőkeacutepesseacuteg javul
sublinguaacutelis nitraacutet felhasznaacutelaacutes csoumlkken
EKG-n az ischaemiaacutes epizoacutedusok csoumlkkennek
ST depresszioacute enyhuumll eacuteletminőseacuteg javul
anginaacutes faacutejdalom csoumlkken
SCS indikaacutecioacutek IIIAngina pectoris
bull tanulmaacutenyok eredmeacutenyei kedvezőek (39-43)
bull teraacutepiaacutes hataacutes hosszuacute taacutevuacute
bull nitraacutet bevitel csoumlkkenthető
bull faacutejdalomcsillapiacutetoacute hataacutesuacute
bull sziacutevizom veacuterkeringeacutes javul
bull PET tanulmaacuteny
ischaemiaacutes sziacutevizomban keringeacuteseacuteben
redistribucio alakul ki nyugalomban
eacutes gyoacutegyszer indukaacutelt stresszben(44)
SCS indikaacutecioacutek IVPerifeacuteriaacutes vasculaacuteris betegseacutegek
bull lassan progrediaacuteloacute perifeacuteriaacutes vasculaacuteris ischaemia -atherosclerosis (Fontaine 3 4 staacutedium )
bull vazospasticus betegseacuteg (pl Raynaud frostbite) gyoacutegyszeresen eacutersebeacuteszeti műteacutettel nem uralhatoacute veacutegtagfaacutejdalom
bull Buerger-koacuter
bull kontraindikaacutelt laacutebszaacuterfekeacutelygt 3 cm gangreacutena
SCS indikaacutecioacutek VCRPS
CRPS tuumlnetei
1 Harden RN et al Pain 199983211-219 6Birklein F et al Pain 19976949-54
2 Galer BS et al J Pain Symptom Manage 200020286-92 7 Schwartzman RJ Kerrigan J
Neurosurgery 19904057-61
3 Birklein F Handwerker HO Pain 2001 941-6 8 Zyluk A J Hand Surg 200126151-154
4 Rommel O et al Pain 19998095-101 9 Wasner G et al Neuro Clin
199816851-68
5 Thimineur M et al Clin J Pain 199814256-67
Sensory Motor dysfunctionIntense pain12 Weakness
Allodynia13 Decreased range of motion3
Hyperesthesia13 Tremor16
Hyperalgesia13 Dystonia7
Sensory deficits4 Myoclonus7
Decreased muscular strength8
Autonomic Dystrophic Swelling1 Increaseddecreased nailhair growth
Colourtemperature changes6 Skin changes (eg palor plantar fibrosis
Sweating abnormalities6 hyperkeratosis and thin glossy
skin9 )
Courtesy of Robert J Schwartzman MD
SCS indikaacutecioacutek VIAbdominaacutelis eacutes visceraacutelis faacutejdalom
szindroacutemaacutek
bull Faacutejdalom etioloacutegiaacuteja vaacuteltozatos
bull Ok gastrointestinaacutelis gastro-urinaacutelis
musculosceletaacutelis idegrendszeri
bull Megfigyeleacutes Th X myelotomia
daganatos pelvicus faacutejdalmat csillapiacutet
Mechanisms of SCS
bull Gate control theory
bull Direct inhibition of spinothalamic neurons
bull Descending modulatory effects
bull Alteration of sympathetic activity
bull Neurochemical modulation
GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

SCS indikaacutecioacutek II
bull Kevert faacutejdalom szindroacutemaacutek
Falied back surgery syndroma = FBSS koraacutebbi gerincsebeacuteszeti beavatkozaacutes (postoperatiacutev fibrosis arachnoiditis)
Posztlaminektomiaacutes szindroacutemaangolszaacutesz failed back surgery szindroacutemaacutenak (FBSS)
bull faacutejdalom lokalizaacutecioacute alsoacute aacutegyeacuteki gerinc far
alsoacute veacutegtagok
bull etioloacutegia arachnoiditis epiduraacutelis heg
radiculitis mikro-instabilitaacutes rec
porckorongseacuterv gyulladaacutes
bull tapasztalatok alsoacute veacutegtagba terjedő
faacutejdalomra SCS hateacutekony
bull axiaacutelis faacutejdalmakra nem bizonyiacutetott
Incidencia FBSS
bull ranges 5 - 50
bull postdiscectomy 10-40
Etiologia FBSS
bull Scar tissue that forms around the surgery site interrupting normal neurological functioning
bull technicalities of the operation are not successful the performing surgeon had poor technique andor there is iatrogenic injury present
bull surgery is not performed at the site that causes the pain
bull surgery performed is not actually necessarybull patient is a poor fit for a successful surgerybull diagnosis was incorrectbull Complications of surgery arise
1 Anderson VC et al Current review of pain 20004105-11 5 Vaccaro AR et al Spine 200126 (24) S111-82 Leveque JC et al Neuromodulation 200141-9 6 Spengler DM et al Spine 19805356-603 Dario A et al Neuromodulation 20014105-110 7 Fager CA Freidberg SR Spine 1980587-944 Ohnmeiss DD et al The Spine Journal 2001358-363 8 Long DM Surgical management of pain 2002 354-64
FBSS okai eacutes tuumlnetei
bull FBSS cause1-7
ndash irreversible nerve injury
ndash surgical complications
ndash psychosocial problems
ndash inappropriate selection of patients for surgery
ndash recurrent herniation
ndash wrong level of operation
bull FBSS symptoms348
ndash lumbosacral postoperative fibrosis andor arachnoiditis
ndash root lesion
ndash dorsal compartment syndrome
ndash lateral spinal stenosis
SCS indikaacutecioacutek IIIAngina pectoris
bull New York Heart Association III-IV csoport (szignifikaacutens coronaacuteria stenosis egy vagy toumlbb szűkuumllet 70 )
bull myocardiaacutelis ischaemia reverzibilis angina gyoacutegyszeres revascularizaacutecioacutes beavatkozaacutesokkal nem enyhiacutethető
bull eacuteletminőseacuteguarr nitro-glicerin felhasznaacutelaacutesdarr anginaacutes rohamok szaacutemadarr jaacuteraacutestaacutevolsaacuteguarr
bull SCS anti-ischaemiaacutes hataacutes
bull nincs bizonyiacuteteacutek SCS hateacutekonysaacutegra instabil angina acut myocardiaacutelis infarctus vazospasticus angia maacutes sziacutevbetegseacuteg okozta anginaacutes faacutejdalmak csillapiacutetaacutesaacutera
Anginaacutes faacutejdalom
SCS tanulmaacutenyok hateacutekonysaacuteg I
bull Nienke (45 ) PT 1 eacutev koumlveteacutes eacuteletminőseacuteg szociaacutelis mentaacutelis fizikaacutelis teljesiacutetmeacuteny szignifikaacutensan javul
bull Hautvast (46) stabil angina pectorisban RT 6 heacutet koumlveteacutes
Randomizaacutelaacutes a stimulaacutetor OFF b csoport 3x1 oacuteranap ON vagy hirtelen anginaacuteban
anginaacutes rohamszaacutem csoumlkken
fizikai teljesiacutetőkeacutepesseacuteg javul
sublinguaacutelis nitraacutet felhasznaacutelaacutes csoumlkken
EKG-n az ischaemiaacutes epizoacutedusok csoumlkkennek
ST depresszioacute enyhuumll eacuteletminőseacuteg javul
anginaacutes faacutejdalom csoumlkken
SCS indikaacutecioacutek IIIAngina pectoris
bull tanulmaacutenyok eredmeacutenyei kedvezőek (39-43)
bull teraacutepiaacutes hataacutes hosszuacute taacutevuacute
bull nitraacutet bevitel csoumlkkenthető
bull faacutejdalomcsillapiacutetoacute hataacutesuacute
bull sziacutevizom veacuterkeringeacutes javul
bull PET tanulmaacuteny
ischaemiaacutes sziacutevizomban keringeacuteseacuteben
redistribucio alakul ki nyugalomban
eacutes gyoacutegyszer indukaacutelt stresszben(44)
SCS indikaacutecioacutek IVPerifeacuteriaacutes vasculaacuteris betegseacutegek
bull lassan progrediaacuteloacute perifeacuteriaacutes vasculaacuteris ischaemia -atherosclerosis (Fontaine 3 4 staacutedium )
bull vazospasticus betegseacuteg (pl Raynaud frostbite) gyoacutegyszeresen eacutersebeacuteszeti műteacutettel nem uralhatoacute veacutegtagfaacutejdalom
bull Buerger-koacuter
bull kontraindikaacutelt laacutebszaacuterfekeacutelygt 3 cm gangreacutena
SCS indikaacutecioacutek VCRPS
CRPS tuumlnetei
1 Harden RN et al Pain 199983211-219 6Birklein F et al Pain 19976949-54
2 Galer BS et al J Pain Symptom Manage 200020286-92 7 Schwartzman RJ Kerrigan J
Neurosurgery 19904057-61
3 Birklein F Handwerker HO Pain 2001 941-6 8 Zyluk A J Hand Surg 200126151-154
4 Rommel O et al Pain 19998095-101 9 Wasner G et al Neuro Clin
199816851-68
5 Thimineur M et al Clin J Pain 199814256-67
Sensory Motor dysfunctionIntense pain12 Weakness
Allodynia13 Decreased range of motion3
Hyperesthesia13 Tremor16
Hyperalgesia13 Dystonia7
Sensory deficits4 Myoclonus7
Decreased muscular strength8
Autonomic Dystrophic Swelling1 Increaseddecreased nailhair growth
Colourtemperature changes6 Skin changes (eg palor plantar fibrosis
Sweating abnormalities6 hyperkeratosis and thin glossy
skin9 )
Courtesy of Robert J Schwartzman MD
SCS indikaacutecioacutek VIAbdominaacutelis eacutes visceraacutelis faacutejdalom
szindroacutemaacutek
bull Faacutejdalom etioloacutegiaacuteja vaacuteltozatos
bull Ok gastrointestinaacutelis gastro-urinaacutelis
musculosceletaacutelis idegrendszeri
bull Megfigyeleacutes Th X myelotomia
daganatos pelvicus faacutejdalmat csillapiacutet
Mechanisms of SCS
bull Gate control theory
bull Direct inhibition of spinothalamic neurons
bull Descending modulatory effects
bull Alteration of sympathetic activity
bull Neurochemical modulation
GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Posztlaminektomiaacutes szindroacutemaangolszaacutesz failed back surgery szindroacutemaacutenak (FBSS)
bull faacutejdalom lokalizaacutecioacute alsoacute aacutegyeacuteki gerinc far
alsoacute veacutegtagok
bull etioloacutegia arachnoiditis epiduraacutelis heg
radiculitis mikro-instabilitaacutes rec
porckorongseacuterv gyulladaacutes
bull tapasztalatok alsoacute veacutegtagba terjedő
faacutejdalomra SCS hateacutekony
bull axiaacutelis faacutejdalmakra nem bizonyiacutetott
Incidencia FBSS
bull ranges 5 - 50
bull postdiscectomy 10-40
Etiologia FBSS
bull Scar tissue that forms around the surgery site interrupting normal neurological functioning
bull technicalities of the operation are not successful the performing surgeon had poor technique andor there is iatrogenic injury present
bull surgery is not performed at the site that causes the pain
bull surgery performed is not actually necessarybull patient is a poor fit for a successful surgerybull diagnosis was incorrectbull Complications of surgery arise
1 Anderson VC et al Current review of pain 20004105-11 5 Vaccaro AR et al Spine 200126 (24) S111-82 Leveque JC et al Neuromodulation 200141-9 6 Spengler DM et al Spine 19805356-603 Dario A et al Neuromodulation 20014105-110 7 Fager CA Freidberg SR Spine 1980587-944 Ohnmeiss DD et al The Spine Journal 2001358-363 8 Long DM Surgical management of pain 2002 354-64
FBSS okai eacutes tuumlnetei
bull FBSS cause1-7
ndash irreversible nerve injury
ndash surgical complications
ndash psychosocial problems
ndash inappropriate selection of patients for surgery
ndash recurrent herniation
ndash wrong level of operation
bull FBSS symptoms348
ndash lumbosacral postoperative fibrosis andor arachnoiditis
ndash root lesion
ndash dorsal compartment syndrome
ndash lateral spinal stenosis
SCS indikaacutecioacutek IIIAngina pectoris
bull New York Heart Association III-IV csoport (szignifikaacutens coronaacuteria stenosis egy vagy toumlbb szűkuumllet 70 )
bull myocardiaacutelis ischaemia reverzibilis angina gyoacutegyszeres revascularizaacutecioacutes beavatkozaacutesokkal nem enyhiacutethető
bull eacuteletminőseacuteguarr nitro-glicerin felhasznaacutelaacutesdarr anginaacutes rohamok szaacutemadarr jaacuteraacutestaacutevolsaacuteguarr
bull SCS anti-ischaemiaacutes hataacutes
bull nincs bizonyiacuteteacutek SCS hateacutekonysaacutegra instabil angina acut myocardiaacutelis infarctus vazospasticus angia maacutes sziacutevbetegseacuteg okozta anginaacutes faacutejdalmak csillapiacutetaacutesaacutera
Anginaacutes faacutejdalom
SCS tanulmaacutenyok hateacutekonysaacuteg I
bull Nienke (45 ) PT 1 eacutev koumlveteacutes eacuteletminőseacuteg szociaacutelis mentaacutelis fizikaacutelis teljesiacutetmeacuteny szignifikaacutensan javul
bull Hautvast (46) stabil angina pectorisban RT 6 heacutet koumlveteacutes
Randomizaacutelaacutes a stimulaacutetor OFF b csoport 3x1 oacuteranap ON vagy hirtelen anginaacuteban
anginaacutes rohamszaacutem csoumlkken
fizikai teljesiacutetőkeacutepesseacuteg javul
sublinguaacutelis nitraacutet felhasznaacutelaacutes csoumlkken
EKG-n az ischaemiaacutes epizoacutedusok csoumlkkennek
ST depresszioacute enyhuumll eacuteletminőseacuteg javul
anginaacutes faacutejdalom csoumlkken
SCS indikaacutecioacutek IIIAngina pectoris
bull tanulmaacutenyok eredmeacutenyei kedvezőek (39-43)
bull teraacutepiaacutes hataacutes hosszuacute taacutevuacute
bull nitraacutet bevitel csoumlkkenthető
bull faacutejdalomcsillapiacutetoacute hataacutesuacute
bull sziacutevizom veacuterkeringeacutes javul
bull PET tanulmaacuteny
ischaemiaacutes sziacutevizomban keringeacuteseacuteben
redistribucio alakul ki nyugalomban
eacutes gyoacutegyszer indukaacutelt stresszben(44)
SCS indikaacutecioacutek IVPerifeacuteriaacutes vasculaacuteris betegseacutegek
bull lassan progrediaacuteloacute perifeacuteriaacutes vasculaacuteris ischaemia -atherosclerosis (Fontaine 3 4 staacutedium )
bull vazospasticus betegseacuteg (pl Raynaud frostbite) gyoacutegyszeresen eacutersebeacuteszeti műteacutettel nem uralhatoacute veacutegtagfaacutejdalom
bull Buerger-koacuter
bull kontraindikaacutelt laacutebszaacuterfekeacutelygt 3 cm gangreacutena
SCS indikaacutecioacutek VCRPS
CRPS tuumlnetei
1 Harden RN et al Pain 199983211-219 6Birklein F et al Pain 19976949-54
2 Galer BS et al J Pain Symptom Manage 200020286-92 7 Schwartzman RJ Kerrigan J
Neurosurgery 19904057-61
3 Birklein F Handwerker HO Pain 2001 941-6 8 Zyluk A J Hand Surg 200126151-154
4 Rommel O et al Pain 19998095-101 9 Wasner G et al Neuro Clin
199816851-68
5 Thimineur M et al Clin J Pain 199814256-67
Sensory Motor dysfunctionIntense pain12 Weakness
Allodynia13 Decreased range of motion3
Hyperesthesia13 Tremor16
Hyperalgesia13 Dystonia7
Sensory deficits4 Myoclonus7
Decreased muscular strength8
Autonomic Dystrophic Swelling1 Increaseddecreased nailhair growth
Colourtemperature changes6 Skin changes (eg palor plantar fibrosis
Sweating abnormalities6 hyperkeratosis and thin glossy
skin9 )
Courtesy of Robert J Schwartzman MD
SCS indikaacutecioacutek VIAbdominaacutelis eacutes visceraacutelis faacutejdalom
szindroacutemaacutek
bull Faacutejdalom etioloacutegiaacuteja vaacuteltozatos
bull Ok gastrointestinaacutelis gastro-urinaacutelis
musculosceletaacutelis idegrendszeri
bull Megfigyeleacutes Th X myelotomia
daganatos pelvicus faacutejdalmat csillapiacutet
Mechanisms of SCS
bull Gate control theory
bull Direct inhibition of spinothalamic neurons
bull Descending modulatory effects
bull Alteration of sympathetic activity
bull Neurochemical modulation
GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Incidencia FBSS
bull ranges 5 - 50
bull postdiscectomy 10-40
Etiologia FBSS
bull Scar tissue that forms around the surgery site interrupting normal neurological functioning
bull technicalities of the operation are not successful the performing surgeon had poor technique andor there is iatrogenic injury present
bull surgery is not performed at the site that causes the pain
bull surgery performed is not actually necessarybull patient is a poor fit for a successful surgerybull diagnosis was incorrectbull Complications of surgery arise
1 Anderson VC et al Current review of pain 20004105-11 5 Vaccaro AR et al Spine 200126 (24) S111-82 Leveque JC et al Neuromodulation 200141-9 6 Spengler DM et al Spine 19805356-603 Dario A et al Neuromodulation 20014105-110 7 Fager CA Freidberg SR Spine 1980587-944 Ohnmeiss DD et al The Spine Journal 2001358-363 8 Long DM Surgical management of pain 2002 354-64
FBSS okai eacutes tuumlnetei
bull FBSS cause1-7
ndash irreversible nerve injury
ndash surgical complications
ndash psychosocial problems
ndash inappropriate selection of patients for surgery
ndash recurrent herniation
ndash wrong level of operation
bull FBSS symptoms348
ndash lumbosacral postoperative fibrosis andor arachnoiditis
ndash root lesion
ndash dorsal compartment syndrome
ndash lateral spinal stenosis
SCS indikaacutecioacutek IIIAngina pectoris
bull New York Heart Association III-IV csoport (szignifikaacutens coronaacuteria stenosis egy vagy toumlbb szűkuumllet 70 )
bull myocardiaacutelis ischaemia reverzibilis angina gyoacutegyszeres revascularizaacutecioacutes beavatkozaacutesokkal nem enyhiacutethető
bull eacuteletminőseacuteguarr nitro-glicerin felhasznaacutelaacutesdarr anginaacutes rohamok szaacutemadarr jaacuteraacutestaacutevolsaacuteguarr
bull SCS anti-ischaemiaacutes hataacutes
bull nincs bizonyiacuteteacutek SCS hateacutekonysaacutegra instabil angina acut myocardiaacutelis infarctus vazospasticus angia maacutes sziacutevbetegseacuteg okozta anginaacutes faacutejdalmak csillapiacutetaacutesaacutera
Anginaacutes faacutejdalom
SCS tanulmaacutenyok hateacutekonysaacuteg I
bull Nienke (45 ) PT 1 eacutev koumlveteacutes eacuteletminőseacuteg szociaacutelis mentaacutelis fizikaacutelis teljesiacutetmeacuteny szignifikaacutensan javul
bull Hautvast (46) stabil angina pectorisban RT 6 heacutet koumlveteacutes
Randomizaacutelaacutes a stimulaacutetor OFF b csoport 3x1 oacuteranap ON vagy hirtelen anginaacuteban
anginaacutes rohamszaacutem csoumlkken
fizikai teljesiacutetőkeacutepesseacuteg javul
sublinguaacutelis nitraacutet felhasznaacutelaacutes csoumlkken
EKG-n az ischaemiaacutes epizoacutedusok csoumlkkennek
ST depresszioacute enyhuumll eacuteletminőseacuteg javul
anginaacutes faacutejdalom csoumlkken
SCS indikaacutecioacutek IIIAngina pectoris
bull tanulmaacutenyok eredmeacutenyei kedvezőek (39-43)
bull teraacutepiaacutes hataacutes hosszuacute taacutevuacute
bull nitraacutet bevitel csoumlkkenthető
bull faacutejdalomcsillapiacutetoacute hataacutesuacute
bull sziacutevizom veacuterkeringeacutes javul
bull PET tanulmaacuteny
ischaemiaacutes sziacutevizomban keringeacuteseacuteben
redistribucio alakul ki nyugalomban
eacutes gyoacutegyszer indukaacutelt stresszben(44)
SCS indikaacutecioacutek IVPerifeacuteriaacutes vasculaacuteris betegseacutegek
bull lassan progrediaacuteloacute perifeacuteriaacutes vasculaacuteris ischaemia -atherosclerosis (Fontaine 3 4 staacutedium )
bull vazospasticus betegseacuteg (pl Raynaud frostbite) gyoacutegyszeresen eacutersebeacuteszeti műteacutettel nem uralhatoacute veacutegtagfaacutejdalom
bull Buerger-koacuter
bull kontraindikaacutelt laacutebszaacuterfekeacutelygt 3 cm gangreacutena
SCS indikaacutecioacutek VCRPS
CRPS tuumlnetei
1 Harden RN et al Pain 199983211-219 6Birklein F et al Pain 19976949-54
2 Galer BS et al J Pain Symptom Manage 200020286-92 7 Schwartzman RJ Kerrigan J
Neurosurgery 19904057-61
3 Birklein F Handwerker HO Pain 2001 941-6 8 Zyluk A J Hand Surg 200126151-154
4 Rommel O et al Pain 19998095-101 9 Wasner G et al Neuro Clin
199816851-68
5 Thimineur M et al Clin J Pain 199814256-67
Sensory Motor dysfunctionIntense pain12 Weakness
Allodynia13 Decreased range of motion3
Hyperesthesia13 Tremor16
Hyperalgesia13 Dystonia7
Sensory deficits4 Myoclonus7
Decreased muscular strength8
Autonomic Dystrophic Swelling1 Increaseddecreased nailhair growth
Colourtemperature changes6 Skin changes (eg palor plantar fibrosis
Sweating abnormalities6 hyperkeratosis and thin glossy
skin9 )
Courtesy of Robert J Schwartzman MD
SCS indikaacutecioacutek VIAbdominaacutelis eacutes visceraacutelis faacutejdalom
szindroacutemaacutek
bull Faacutejdalom etioloacutegiaacuteja vaacuteltozatos
bull Ok gastrointestinaacutelis gastro-urinaacutelis
musculosceletaacutelis idegrendszeri
bull Megfigyeleacutes Th X myelotomia
daganatos pelvicus faacutejdalmat csillapiacutet
Mechanisms of SCS
bull Gate control theory
bull Direct inhibition of spinothalamic neurons
bull Descending modulatory effects
bull Alteration of sympathetic activity
bull Neurochemical modulation
GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Etiologia FBSS
bull Scar tissue that forms around the surgery site interrupting normal neurological functioning
bull technicalities of the operation are not successful the performing surgeon had poor technique andor there is iatrogenic injury present
bull surgery is not performed at the site that causes the pain
bull surgery performed is not actually necessarybull patient is a poor fit for a successful surgerybull diagnosis was incorrectbull Complications of surgery arise
1 Anderson VC et al Current review of pain 20004105-11 5 Vaccaro AR et al Spine 200126 (24) S111-82 Leveque JC et al Neuromodulation 200141-9 6 Spengler DM et al Spine 19805356-603 Dario A et al Neuromodulation 20014105-110 7 Fager CA Freidberg SR Spine 1980587-944 Ohnmeiss DD et al The Spine Journal 2001358-363 8 Long DM Surgical management of pain 2002 354-64
FBSS okai eacutes tuumlnetei
bull FBSS cause1-7
ndash irreversible nerve injury
ndash surgical complications
ndash psychosocial problems
ndash inappropriate selection of patients for surgery
ndash recurrent herniation
ndash wrong level of operation
bull FBSS symptoms348
ndash lumbosacral postoperative fibrosis andor arachnoiditis
ndash root lesion
ndash dorsal compartment syndrome
ndash lateral spinal stenosis
SCS indikaacutecioacutek IIIAngina pectoris
bull New York Heart Association III-IV csoport (szignifikaacutens coronaacuteria stenosis egy vagy toumlbb szűkuumllet 70 )
bull myocardiaacutelis ischaemia reverzibilis angina gyoacutegyszeres revascularizaacutecioacutes beavatkozaacutesokkal nem enyhiacutethető
bull eacuteletminőseacuteguarr nitro-glicerin felhasznaacutelaacutesdarr anginaacutes rohamok szaacutemadarr jaacuteraacutestaacutevolsaacuteguarr
bull SCS anti-ischaemiaacutes hataacutes
bull nincs bizonyiacuteteacutek SCS hateacutekonysaacutegra instabil angina acut myocardiaacutelis infarctus vazospasticus angia maacutes sziacutevbetegseacuteg okozta anginaacutes faacutejdalmak csillapiacutetaacutesaacutera
Anginaacutes faacutejdalom
SCS tanulmaacutenyok hateacutekonysaacuteg I
bull Nienke (45 ) PT 1 eacutev koumlveteacutes eacuteletminőseacuteg szociaacutelis mentaacutelis fizikaacutelis teljesiacutetmeacuteny szignifikaacutensan javul
bull Hautvast (46) stabil angina pectorisban RT 6 heacutet koumlveteacutes
Randomizaacutelaacutes a stimulaacutetor OFF b csoport 3x1 oacuteranap ON vagy hirtelen anginaacuteban
anginaacutes rohamszaacutem csoumlkken
fizikai teljesiacutetőkeacutepesseacuteg javul
sublinguaacutelis nitraacutet felhasznaacutelaacutes csoumlkken
EKG-n az ischaemiaacutes epizoacutedusok csoumlkkennek
ST depresszioacute enyhuumll eacuteletminőseacuteg javul
anginaacutes faacutejdalom csoumlkken
SCS indikaacutecioacutek IIIAngina pectoris
bull tanulmaacutenyok eredmeacutenyei kedvezőek (39-43)
bull teraacutepiaacutes hataacutes hosszuacute taacutevuacute
bull nitraacutet bevitel csoumlkkenthető
bull faacutejdalomcsillapiacutetoacute hataacutesuacute
bull sziacutevizom veacuterkeringeacutes javul
bull PET tanulmaacuteny
ischaemiaacutes sziacutevizomban keringeacuteseacuteben
redistribucio alakul ki nyugalomban
eacutes gyoacutegyszer indukaacutelt stresszben(44)
SCS indikaacutecioacutek IVPerifeacuteriaacutes vasculaacuteris betegseacutegek
bull lassan progrediaacuteloacute perifeacuteriaacutes vasculaacuteris ischaemia -atherosclerosis (Fontaine 3 4 staacutedium )
bull vazospasticus betegseacuteg (pl Raynaud frostbite) gyoacutegyszeresen eacutersebeacuteszeti műteacutettel nem uralhatoacute veacutegtagfaacutejdalom
bull Buerger-koacuter
bull kontraindikaacutelt laacutebszaacuterfekeacutelygt 3 cm gangreacutena
SCS indikaacutecioacutek VCRPS
CRPS tuumlnetei
1 Harden RN et al Pain 199983211-219 6Birklein F et al Pain 19976949-54
2 Galer BS et al J Pain Symptom Manage 200020286-92 7 Schwartzman RJ Kerrigan J
Neurosurgery 19904057-61
3 Birklein F Handwerker HO Pain 2001 941-6 8 Zyluk A J Hand Surg 200126151-154
4 Rommel O et al Pain 19998095-101 9 Wasner G et al Neuro Clin
199816851-68
5 Thimineur M et al Clin J Pain 199814256-67
Sensory Motor dysfunctionIntense pain12 Weakness
Allodynia13 Decreased range of motion3
Hyperesthesia13 Tremor16
Hyperalgesia13 Dystonia7
Sensory deficits4 Myoclonus7
Decreased muscular strength8
Autonomic Dystrophic Swelling1 Increaseddecreased nailhair growth
Colourtemperature changes6 Skin changes (eg palor plantar fibrosis
Sweating abnormalities6 hyperkeratosis and thin glossy
skin9 )
Courtesy of Robert J Schwartzman MD
SCS indikaacutecioacutek VIAbdominaacutelis eacutes visceraacutelis faacutejdalom
szindroacutemaacutek
bull Faacutejdalom etioloacutegiaacuteja vaacuteltozatos
bull Ok gastrointestinaacutelis gastro-urinaacutelis
musculosceletaacutelis idegrendszeri
bull Megfigyeleacutes Th X myelotomia
daganatos pelvicus faacutejdalmat csillapiacutet
Mechanisms of SCS
bull Gate control theory
bull Direct inhibition of spinothalamic neurons
bull Descending modulatory effects
bull Alteration of sympathetic activity
bull Neurochemical modulation
GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

1 Anderson VC et al Current review of pain 20004105-11 5 Vaccaro AR et al Spine 200126 (24) S111-82 Leveque JC et al Neuromodulation 200141-9 6 Spengler DM et al Spine 19805356-603 Dario A et al Neuromodulation 20014105-110 7 Fager CA Freidberg SR Spine 1980587-944 Ohnmeiss DD et al The Spine Journal 2001358-363 8 Long DM Surgical management of pain 2002 354-64
FBSS okai eacutes tuumlnetei
bull FBSS cause1-7
ndash irreversible nerve injury
ndash surgical complications
ndash psychosocial problems
ndash inappropriate selection of patients for surgery
ndash recurrent herniation
ndash wrong level of operation
bull FBSS symptoms348
ndash lumbosacral postoperative fibrosis andor arachnoiditis
ndash root lesion
ndash dorsal compartment syndrome
ndash lateral spinal stenosis
SCS indikaacutecioacutek IIIAngina pectoris
bull New York Heart Association III-IV csoport (szignifikaacutens coronaacuteria stenosis egy vagy toumlbb szűkuumllet 70 )
bull myocardiaacutelis ischaemia reverzibilis angina gyoacutegyszeres revascularizaacutecioacutes beavatkozaacutesokkal nem enyhiacutethető
bull eacuteletminőseacuteguarr nitro-glicerin felhasznaacutelaacutesdarr anginaacutes rohamok szaacutemadarr jaacuteraacutestaacutevolsaacuteguarr
bull SCS anti-ischaemiaacutes hataacutes
bull nincs bizonyiacuteteacutek SCS hateacutekonysaacutegra instabil angina acut myocardiaacutelis infarctus vazospasticus angia maacutes sziacutevbetegseacuteg okozta anginaacutes faacutejdalmak csillapiacutetaacutesaacutera
Anginaacutes faacutejdalom
SCS tanulmaacutenyok hateacutekonysaacuteg I
bull Nienke (45 ) PT 1 eacutev koumlveteacutes eacuteletminőseacuteg szociaacutelis mentaacutelis fizikaacutelis teljesiacutetmeacuteny szignifikaacutensan javul
bull Hautvast (46) stabil angina pectorisban RT 6 heacutet koumlveteacutes
Randomizaacutelaacutes a stimulaacutetor OFF b csoport 3x1 oacuteranap ON vagy hirtelen anginaacuteban
anginaacutes rohamszaacutem csoumlkken
fizikai teljesiacutetőkeacutepesseacuteg javul
sublinguaacutelis nitraacutet felhasznaacutelaacutes csoumlkken
EKG-n az ischaemiaacutes epizoacutedusok csoumlkkennek
ST depresszioacute enyhuumll eacuteletminőseacuteg javul
anginaacutes faacutejdalom csoumlkken
SCS indikaacutecioacutek IIIAngina pectoris
bull tanulmaacutenyok eredmeacutenyei kedvezőek (39-43)
bull teraacutepiaacutes hataacutes hosszuacute taacutevuacute
bull nitraacutet bevitel csoumlkkenthető
bull faacutejdalomcsillapiacutetoacute hataacutesuacute
bull sziacutevizom veacuterkeringeacutes javul
bull PET tanulmaacuteny
ischaemiaacutes sziacutevizomban keringeacuteseacuteben
redistribucio alakul ki nyugalomban
eacutes gyoacutegyszer indukaacutelt stresszben(44)
SCS indikaacutecioacutek IVPerifeacuteriaacutes vasculaacuteris betegseacutegek
bull lassan progrediaacuteloacute perifeacuteriaacutes vasculaacuteris ischaemia -atherosclerosis (Fontaine 3 4 staacutedium )
bull vazospasticus betegseacuteg (pl Raynaud frostbite) gyoacutegyszeresen eacutersebeacuteszeti műteacutettel nem uralhatoacute veacutegtagfaacutejdalom
bull Buerger-koacuter
bull kontraindikaacutelt laacutebszaacuterfekeacutelygt 3 cm gangreacutena
SCS indikaacutecioacutek VCRPS
CRPS tuumlnetei
1 Harden RN et al Pain 199983211-219 6Birklein F et al Pain 19976949-54
2 Galer BS et al J Pain Symptom Manage 200020286-92 7 Schwartzman RJ Kerrigan J
Neurosurgery 19904057-61
3 Birklein F Handwerker HO Pain 2001 941-6 8 Zyluk A J Hand Surg 200126151-154
4 Rommel O et al Pain 19998095-101 9 Wasner G et al Neuro Clin
199816851-68
5 Thimineur M et al Clin J Pain 199814256-67
Sensory Motor dysfunctionIntense pain12 Weakness
Allodynia13 Decreased range of motion3
Hyperesthesia13 Tremor16
Hyperalgesia13 Dystonia7
Sensory deficits4 Myoclonus7
Decreased muscular strength8
Autonomic Dystrophic Swelling1 Increaseddecreased nailhair growth
Colourtemperature changes6 Skin changes (eg palor plantar fibrosis
Sweating abnormalities6 hyperkeratosis and thin glossy
skin9 )
Courtesy of Robert J Schwartzman MD
SCS indikaacutecioacutek VIAbdominaacutelis eacutes visceraacutelis faacutejdalom
szindroacutemaacutek
bull Faacutejdalom etioloacutegiaacuteja vaacuteltozatos
bull Ok gastrointestinaacutelis gastro-urinaacutelis
musculosceletaacutelis idegrendszeri
bull Megfigyeleacutes Th X myelotomia
daganatos pelvicus faacutejdalmat csillapiacutet
Mechanisms of SCS
bull Gate control theory
bull Direct inhibition of spinothalamic neurons
bull Descending modulatory effects
bull Alteration of sympathetic activity
bull Neurochemical modulation
GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

SCS indikaacutecioacutek IIIAngina pectoris
bull New York Heart Association III-IV csoport (szignifikaacutens coronaacuteria stenosis egy vagy toumlbb szűkuumllet 70 )
bull myocardiaacutelis ischaemia reverzibilis angina gyoacutegyszeres revascularizaacutecioacutes beavatkozaacutesokkal nem enyhiacutethető
bull eacuteletminőseacuteguarr nitro-glicerin felhasznaacutelaacutesdarr anginaacutes rohamok szaacutemadarr jaacuteraacutestaacutevolsaacuteguarr
bull SCS anti-ischaemiaacutes hataacutes
bull nincs bizonyiacuteteacutek SCS hateacutekonysaacutegra instabil angina acut myocardiaacutelis infarctus vazospasticus angia maacutes sziacutevbetegseacuteg okozta anginaacutes faacutejdalmak csillapiacutetaacutesaacutera
Anginaacutes faacutejdalom
SCS tanulmaacutenyok hateacutekonysaacuteg I
bull Nienke (45 ) PT 1 eacutev koumlveteacutes eacuteletminőseacuteg szociaacutelis mentaacutelis fizikaacutelis teljesiacutetmeacuteny szignifikaacutensan javul
bull Hautvast (46) stabil angina pectorisban RT 6 heacutet koumlveteacutes
Randomizaacutelaacutes a stimulaacutetor OFF b csoport 3x1 oacuteranap ON vagy hirtelen anginaacuteban
anginaacutes rohamszaacutem csoumlkken
fizikai teljesiacutetőkeacutepesseacuteg javul
sublinguaacutelis nitraacutet felhasznaacutelaacutes csoumlkken
EKG-n az ischaemiaacutes epizoacutedusok csoumlkkennek
ST depresszioacute enyhuumll eacuteletminőseacuteg javul
anginaacutes faacutejdalom csoumlkken
SCS indikaacutecioacutek IIIAngina pectoris
bull tanulmaacutenyok eredmeacutenyei kedvezőek (39-43)
bull teraacutepiaacutes hataacutes hosszuacute taacutevuacute
bull nitraacutet bevitel csoumlkkenthető
bull faacutejdalomcsillapiacutetoacute hataacutesuacute
bull sziacutevizom veacuterkeringeacutes javul
bull PET tanulmaacuteny
ischaemiaacutes sziacutevizomban keringeacuteseacuteben
redistribucio alakul ki nyugalomban
eacutes gyoacutegyszer indukaacutelt stresszben(44)
SCS indikaacutecioacutek IVPerifeacuteriaacutes vasculaacuteris betegseacutegek
bull lassan progrediaacuteloacute perifeacuteriaacutes vasculaacuteris ischaemia -atherosclerosis (Fontaine 3 4 staacutedium )
bull vazospasticus betegseacuteg (pl Raynaud frostbite) gyoacutegyszeresen eacutersebeacuteszeti műteacutettel nem uralhatoacute veacutegtagfaacutejdalom
bull Buerger-koacuter
bull kontraindikaacutelt laacutebszaacuterfekeacutelygt 3 cm gangreacutena
SCS indikaacutecioacutek VCRPS
CRPS tuumlnetei
1 Harden RN et al Pain 199983211-219 6Birklein F et al Pain 19976949-54
2 Galer BS et al J Pain Symptom Manage 200020286-92 7 Schwartzman RJ Kerrigan J
Neurosurgery 19904057-61
3 Birklein F Handwerker HO Pain 2001 941-6 8 Zyluk A J Hand Surg 200126151-154
4 Rommel O et al Pain 19998095-101 9 Wasner G et al Neuro Clin
199816851-68
5 Thimineur M et al Clin J Pain 199814256-67
Sensory Motor dysfunctionIntense pain12 Weakness
Allodynia13 Decreased range of motion3
Hyperesthesia13 Tremor16
Hyperalgesia13 Dystonia7
Sensory deficits4 Myoclonus7
Decreased muscular strength8
Autonomic Dystrophic Swelling1 Increaseddecreased nailhair growth
Colourtemperature changes6 Skin changes (eg palor plantar fibrosis
Sweating abnormalities6 hyperkeratosis and thin glossy
skin9 )
Courtesy of Robert J Schwartzman MD
SCS indikaacutecioacutek VIAbdominaacutelis eacutes visceraacutelis faacutejdalom
szindroacutemaacutek
bull Faacutejdalom etioloacutegiaacuteja vaacuteltozatos
bull Ok gastrointestinaacutelis gastro-urinaacutelis
musculosceletaacutelis idegrendszeri
bull Megfigyeleacutes Th X myelotomia
daganatos pelvicus faacutejdalmat csillapiacutet
Mechanisms of SCS
bull Gate control theory
bull Direct inhibition of spinothalamic neurons
bull Descending modulatory effects
bull Alteration of sympathetic activity
bull Neurochemical modulation
GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Anginaacutes faacutejdalom
SCS tanulmaacutenyok hateacutekonysaacuteg I
bull Nienke (45 ) PT 1 eacutev koumlveteacutes eacuteletminőseacuteg szociaacutelis mentaacutelis fizikaacutelis teljesiacutetmeacuteny szignifikaacutensan javul
bull Hautvast (46) stabil angina pectorisban RT 6 heacutet koumlveteacutes
Randomizaacutelaacutes a stimulaacutetor OFF b csoport 3x1 oacuteranap ON vagy hirtelen anginaacuteban
anginaacutes rohamszaacutem csoumlkken
fizikai teljesiacutetőkeacutepesseacuteg javul
sublinguaacutelis nitraacutet felhasznaacutelaacutes csoumlkken
EKG-n az ischaemiaacutes epizoacutedusok csoumlkkennek
ST depresszioacute enyhuumll eacuteletminőseacuteg javul
anginaacutes faacutejdalom csoumlkken
SCS indikaacutecioacutek IIIAngina pectoris
bull tanulmaacutenyok eredmeacutenyei kedvezőek (39-43)
bull teraacutepiaacutes hataacutes hosszuacute taacutevuacute
bull nitraacutet bevitel csoumlkkenthető
bull faacutejdalomcsillapiacutetoacute hataacutesuacute
bull sziacutevizom veacuterkeringeacutes javul
bull PET tanulmaacuteny
ischaemiaacutes sziacutevizomban keringeacuteseacuteben
redistribucio alakul ki nyugalomban
eacutes gyoacutegyszer indukaacutelt stresszben(44)
SCS indikaacutecioacutek IVPerifeacuteriaacutes vasculaacuteris betegseacutegek
bull lassan progrediaacuteloacute perifeacuteriaacutes vasculaacuteris ischaemia -atherosclerosis (Fontaine 3 4 staacutedium )
bull vazospasticus betegseacuteg (pl Raynaud frostbite) gyoacutegyszeresen eacutersebeacuteszeti műteacutettel nem uralhatoacute veacutegtagfaacutejdalom
bull Buerger-koacuter
bull kontraindikaacutelt laacutebszaacuterfekeacutelygt 3 cm gangreacutena
SCS indikaacutecioacutek VCRPS
CRPS tuumlnetei
1 Harden RN et al Pain 199983211-219 6Birklein F et al Pain 19976949-54
2 Galer BS et al J Pain Symptom Manage 200020286-92 7 Schwartzman RJ Kerrigan J
Neurosurgery 19904057-61
3 Birklein F Handwerker HO Pain 2001 941-6 8 Zyluk A J Hand Surg 200126151-154
4 Rommel O et al Pain 19998095-101 9 Wasner G et al Neuro Clin
199816851-68
5 Thimineur M et al Clin J Pain 199814256-67
Sensory Motor dysfunctionIntense pain12 Weakness
Allodynia13 Decreased range of motion3
Hyperesthesia13 Tremor16
Hyperalgesia13 Dystonia7
Sensory deficits4 Myoclonus7
Decreased muscular strength8
Autonomic Dystrophic Swelling1 Increaseddecreased nailhair growth
Colourtemperature changes6 Skin changes (eg palor plantar fibrosis
Sweating abnormalities6 hyperkeratosis and thin glossy
skin9 )
Courtesy of Robert J Schwartzman MD
SCS indikaacutecioacutek VIAbdominaacutelis eacutes visceraacutelis faacutejdalom
szindroacutemaacutek
bull Faacutejdalom etioloacutegiaacuteja vaacuteltozatos
bull Ok gastrointestinaacutelis gastro-urinaacutelis
musculosceletaacutelis idegrendszeri
bull Megfigyeleacutes Th X myelotomia
daganatos pelvicus faacutejdalmat csillapiacutet
Mechanisms of SCS
bull Gate control theory
bull Direct inhibition of spinothalamic neurons
bull Descending modulatory effects
bull Alteration of sympathetic activity
bull Neurochemical modulation
GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

SCS indikaacutecioacutek IIIAngina pectoris
bull tanulmaacutenyok eredmeacutenyei kedvezőek (39-43)
bull teraacutepiaacutes hataacutes hosszuacute taacutevuacute
bull nitraacutet bevitel csoumlkkenthető
bull faacutejdalomcsillapiacutetoacute hataacutesuacute
bull sziacutevizom veacuterkeringeacutes javul
bull PET tanulmaacuteny
ischaemiaacutes sziacutevizomban keringeacuteseacuteben
redistribucio alakul ki nyugalomban
eacutes gyoacutegyszer indukaacutelt stresszben(44)
SCS indikaacutecioacutek IVPerifeacuteriaacutes vasculaacuteris betegseacutegek
bull lassan progrediaacuteloacute perifeacuteriaacutes vasculaacuteris ischaemia -atherosclerosis (Fontaine 3 4 staacutedium )
bull vazospasticus betegseacuteg (pl Raynaud frostbite) gyoacutegyszeresen eacutersebeacuteszeti műteacutettel nem uralhatoacute veacutegtagfaacutejdalom
bull Buerger-koacuter
bull kontraindikaacutelt laacutebszaacuterfekeacutelygt 3 cm gangreacutena
SCS indikaacutecioacutek VCRPS
CRPS tuumlnetei
1 Harden RN et al Pain 199983211-219 6Birklein F et al Pain 19976949-54
2 Galer BS et al J Pain Symptom Manage 200020286-92 7 Schwartzman RJ Kerrigan J
Neurosurgery 19904057-61
3 Birklein F Handwerker HO Pain 2001 941-6 8 Zyluk A J Hand Surg 200126151-154
4 Rommel O et al Pain 19998095-101 9 Wasner G et al Neuro Clin
199816851-68
5 Thimineur M et al Clin J Pain 199814256-67
Sensory Motor dysfunctionIntense pain12 Weakness
Allodynia13 Decreased range of motion3
Hyperesthesia13 Tremor16
Hyperalgesia13 Dystonia7
Sensory deficits4 Myoclonus7
Decreased muscular strength8
Autonomic Dystrophic Swelling1 Increaseddecreased nailhair growth
Colourtemperature changes6 Skin changes (eg palor plantar fibrosis
Sweating abnormalities6 hyperkeratosis and thin glossy
skin9 )
Courtesy of Robert J Schwartzman MD
SCS indikaacutecioacutek VIAbdominaacutelis eacutes visceraacutelis faacutejdalom
szindroacutemaacutek
bull Faacutejdalom etioloacutegiaacuteja vaacuteltozatos
bull Ok gastrointestinaacutelis gastro-urinaacutelis
musculosceletaacutelis idegrendszeri
bull Megfigyeleacutes Th X myelotomia
daganatos pelvicus faacutejdalmat csillapiacutet
Mechanisms of SCS
bull Gate control theory
bull Direct inhibition of spinothalamic neurons
bull Descending modulatory effects
bull Alteration of sympathetic activity
bull Neurochemical modulation
GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

SCS indikaacutecioacutek IVPerifeacuteriaacutes vasculaacuteris betegseacutegek
bull lassan progrediaacuteloacute perifeacuteriaacutes vasculaacuteris ischaemia -atherosclerosis (Fontaine 3 4 staacutedium )
bull vazospasticus betegseacuteg (pl Raynaud frostbite) gyoacutegyszeresen eacutersebeacuteszeti műteacutettel nem uralhatoacute veacutegtagfaacutejdalom
bull Buerger-koacuter
bull kontraindikaacutelt laacutebszaacuterfekeacutelygt 3 cm gangreacutena
SCS indikaacutecioacutek VCRPS
CRPS tuumlnetei
1 Harden RN et al Pain 199983211-219 6Birklein F et al Pain 19976949-54
2 Galer BS et al J Pain Symptom Manage 200020286-92 7 Schwartzman RJ Kerrigan J
Neurosurgery 19904057-61
3 Birklein F Handwerker HO Pain 2001 941-6 8 Zyluk A J Hand Surg 200126151-154
4 Rommel O et al Pain 19998095-101 9 Wasner G et al Neuro Clin
199816851-68
5 Thimineur M et al Clin J Pain 199814256-67
Sensory Motor dysfunctionIntense pain12 Weakness
Allodynia13 Decreased range of motion3
Hyperesthesia13 Tremor16
Hyperalgesia13 Dystonia7
Sensory deficits4 Myoclonus7
Decreased muscular strength8
Autonomic Dystrophic Swelling1 Increaseddecreased nailhair growth
Colourtemperature changes6 Skin changes (eg palor plantar fibrosis
Sweating abnormalities6 hyperkeratosis and thin glossy
skin9 )
Courtesy of Robert J Schwartzman MD
SCS indikaacutecioacutek VIAbdominaacutelis eacutes visceraacutelis faacutejdalom
szindroacutemaacutek
bull Faacutejdalom etioloacutegiaacuteja vaacuteltozatos
bull Ok gastrointestinaacutelis gastro-urinaacutelis
musculosceletaacutelis idegrendszeri
bull Megfigyeleacutes Th X myelotomia
daganatos pelvicus faacutejdalmat csillapiacutet
Mechanisms of SCS
bull Gate control theory
bull Direct inhibition of spinothalamic neurons
bull Descending modulatory effects
bull Alteration of sympathetic activity
bull Neurochemical modulation
GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

SCS indikaacutecioacutek VCRPS
CRPS tuumlnetei
1 Harden RN et al Pain 199983211-219 6Birklein F et al Pain 19976949-54
2 Galer BS et al J Pain Symptom Manage 200020286-92 7 Schwartzman RJ Kerrigan J
Neurosurgery 19904057-61
3 Birklein F Handwerker HO Pain 2001 941-6 8 Zyluk A J Hand Surg 200126151-154
4 Rommel O et al Pain 19998095-101 9 Wasner G et al Neuro Clin
199816851-68
5 Thimineur M et al Clin J Pain 199814256-67
Sensory Motor dysfunctionIntense pain12 Weakness
Allodynia13 Decreased range of motion3
Hyperesthesia13 Tremor16
Hyperalgesia13 Dystonia7
Sensory deficits4 Myoclonus7
Decreased muscular strength8
Autonomic Dystrophic Swelling1 Increaseddecreased nailhair growth
Colourtemperature changes6 Skin changes (eg palor plantar fibrosis
Sweating abnormalities6 hyperkeratosis and thin glossy
skin9 )
Courtesy of Robert J Schwartzman MD
SCS indikaacutecioacutek VIAbdominaacutelis eacutes visceraacutelis faacutejdalom
szindroacutemaacutek
bull Faacutejdalom etioloacutegiaacuteja vaacuteltozatos
bull Ok gastrointestinaacutelis gastro-urinaacutelis
musculosceletaacutelis idegrendszeri
bull Megfigyeleacutes Th X myelotomia
daganatos pelvicus faacutejdalmat csillapiacutet
Mechanisms of SCS
bull Gate control theory
bull Direct inhibition of spinothalamic neurons
bull Descending modulatory effects
bull Alteration of sympathetic activity
bull Neurochemical modulation
GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

CRPS tuumlnetei
1 Harden RN et al Pain 199983211-219 6Birklein F et al Pain 19976949-54
2 Galer BS et al J Pain Symptom Manage 200020286-92 7 Schwartzman RJ Kerrigan J
Neurosurgery 19904057-61
3 Birklein F Handwerker HO Pain 2001 941-6 8 Zyluk A J Hand Surg 200126151-154
4 Rommel O et al Pain 19998095-101 9 Wasner G et al Neuro Clin
199816851-68
5 Thimineur M et al Clin J Pain 199814256-67
Sensory Motor dysfunctionIntense pain12 Weakness
Allodynia13 Decreased range of motion3
Hyperesthesia13 Tremor16
Hyperalgesia13 Dystonia7
Sensory deficits4 Myoclonus7
Decreased muscular strength8
Autonomic Dystrophic Swelling1 Increaseddecreased nailhair growth
Colourtemperature changes6 Skin changes (eg palor plantar fibrosis
Sweating abnormalities6 hyperkeratosis and thin glossy
skin9 )
Courtesy of Robert J Schwartzman MD
SCS indikaacutecioacutek VIAbdominaacutelis eacutes visceraacutelis faacutejdalom
szindroacutemaacutek
bull Faacutejdalom etioloacutegiaacuteja vaacuteltozatos
bull Ok gastrointestinaacutelis gastro-urinaacutelis
musculosceletaacutelis idegrendszeri
bull Megfigyeleacutes Th X myelotomia
daganatos pelvicus faacutejdalmat csillapiacutet
Mechanisms of SCS
bull Gate control theory
bull Direct inhibition of spinothalamic neurons
bull Descending modulatory effects
bull Alteration of sympathetic activity
bull Neurochemical modulation
GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

SCS indikaacutecioacutek VIAbdominaacutelis eacutes visceraacutelis faacutejdalom
szindroacutemaacutek
bull Faacutejdalom etioloacutegiaacuteja vaacuteltozatos
bull Ok gastrointestinaacutelis gastro-urinaacutelis
musculosceletaacutelis idegrendszeri
bull Megfigyeleacutes Th X myelotomia
daganatos pelvicus faacutejdalmat csillapiacutet
Mechanisms of SCS
bull Gate control theory
bull Direct inhibition of spinothalamic neurons
bull Descending modulatory effects
bull Alteration of sympathetic activity
bull Neurochemical modulation
GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Mechanisms of SCS
bull Gate control theory
bull Direct inhibition of spinothalamic neurons
bull Descending modulatory effects
bull Alteration of sympathetic activity
bull Neurochemical modulation
GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

GATE CONTROL THEORYRon Melzack amp Patrick Wall 1967
SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

SCS mechanisms of actionWolter T et al November 2014 Volume 20147 Pages 651mdash663
httpdxdoiorg102147JPRS37589
bull gate control theory nociceptive signal in the dorsal horn would be inhibited by antidromicactivation of collateral fibers of the dorsal columns This explanation only partially true (only a little knowledge about supraspinalcontrol of pain transmission and SCS was thought to act at the segmental level15)
bull wide dynamic range (WDR) neurons in the dorsal horn (convergent multireceptive)
SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

SCS mechanisms of actionbull Overexcitability of WDR neurons in the dorsal horn can be
overcome by SCS16
bull related to an increased basal release of glutamate and to a dysfunction of (GABA) system in animals
bull SCS decreased extracellular glutamate concentration in the dorsal horn18
bull activation of the GABAB receptor play a crucial role18ndash20
bull Release of acetylcholine under SCS bull activation of the M4 muscarine receptor21 muscarine
receptor agonists led to amplification of the SCS effects in rats22
bull serotonergic pain-modulating descending pathways were involved in this effect23
bull SCS inhibited wind-up in the WDR neurons whereas stimulation of the spinal ganglia did not Guan et al27
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom I
bull Melzak eacutes Wall 1965 bdquokaputeoacuteriardquovastag myelinizaacutelt bdquoArdquo rostok ingerleacutese gaacutetolja a transmissioacutet a veacutekony myelin neacutelkuumlli bdquoCrdquo primer afferens rostokban Epiduraacutelis elektroacuteda stimulaacutelja a haacutetsoacute koumlteget ami gaacutetolja vagy modulaacutelja a bejoumlvő nociceptiacutev inputot a veacutekony rostokban
bull Ruhston 2002 SCS a haacutetsoacuteszarvi neuronokat radiculusokat eacutes haacutetsoacute koumltelet is aktivaacuteljaTractus spinothalamicus transmissio gaacutetlaacutesa
centraacutelis gaacutetloacutemechanizmusok aktivaacutelaacutesa reacuteveacuten sympaticus efferens neuronok koumlzvetiacuteteacuteseacutevelgaacutetloacute neurotransmitterek reacuteveacuten
CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

CSC hataacutesmechanizmusNeuropathiaacutes faacutejdalom
bull Stojanovic 2001 haacutetsoacute szarvi neuronok aktivitaacutesaacutet gaacutetolja
bull Cui 1997 fokozza a GABA haacutetsoacute szarvra kifejtett gaacutetloacute hataacutesaacutet
bull Meyerson 1997 intrathecalis GABA agonista(baclofen) fokozza az SCS hataacutesaacutet
adenozin faacutejdalomcsillapiacutetoacute paacutelyaacutek disinhibicioacuteja a periaqueductalis szuumlrkeaacutellomaacutenyban
bull Linderot 1992 Meyerson 2000 fokozza a serotonineacutes substance P felszabadulaacutest
Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Pain 1996 Aug66(2-3)287-95Effects of spinal cord stimulation on touch-evoked allodynia involve GABAergic mechanisms An
experimental study in the mononeuropathic ratCui JG Linderoth B Meyerson BA
bull in mononeuropathic animals with definite signs of tactile allodynia which did not respond to SCS GABA-A and the GABAB-agonist baclofen were administered intrathecally
bull SCS may operate by upgrading the spinal GABAergic
bull effects of SCS are more linked to GABAB-than to GABAA-receptor system
Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Eur J Pain 2008 Jan12(1)132-6 Epub 2007 May 1Baclofen-enhanced spinal cord stimulation and intrathecal baclofen alone for neuropathic pain Long-term outcome of
a pilot studyLind G Schechtmann G Winter J Meyerson BA Linderoth B
intrathecal baclofen (GABA-B receptor agonist) delivery together with SCS
deficient SCS effect in neuropathic pain considerably improved by intrathecal baclofen administration enhanced effect persists for a long-time
Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Spine 2008 Feb 1533(4)E90-3Neurophysiological evidence of antidromic activation of large myelinated fibres in lower limbs during spinal
cord stimulationBuonocore M Bonezzi C Barolat G
bull Perifeacuteriaacutes idegek antidroacutemos aktivaacutecioacuteja
CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

CSC hataacutesmechanizmus PVD-ben
bull Linderot 1999 Kemler 2000 oxigeacuten ellaacutetaacutes reballansziacuterozaacutesaacuteval megelőzi az ischaemiaacutet
Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Test stimulation
bull full paresthesia coverage of the painful area
bull test phase 6ndash12 days
bull decision whether or not to implant an IPG
bull more than 50 pain reduction
bull quality of life and moods are improved
bull analgetic medication can be reduced
bull patient wants the implant
Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Patient selectionscreening includingpsychological
bull some patients do not profit from SCS (17ndash20) negative trial result28)
bull SCS effects diminish over time electrodeproblems (dislocation breakage) psychological factors
bull negative correlation between the level of depression and SCS efficacy3132
bull Demand for technological developments
Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Stimulation Modes
Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Conventional stimulation
SCS using biphasic (40-100 Hz) below 300 Hz
previously considered to be the highest physiological response rate of neural tissue (22)
Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Current technological development
Burst stimulation
bull ldquoburstsrdquo of 5 impulses of 1 ms duration followed by a 1 ms interval applied at a frequency of 500 Hz
bull pain was strongly relieved compared with conventional stimulation
bull no stimulation-induced paresthesia necessary to obtain a pain-relieving effect
bull leg pain also back pain was relieved3435
Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Current technological development
High-frequency (kilohertz) stimulation
bull continuous stimulation with 10 kHz
bull prospective multicenter study favorableresults36
bull radicular leg pain also back pain
bull results stable after 24 months37
bull no paresthesia is perceived (desensitization of hyperactive WDR neurons and control of wind-up phenomenon of WDR neurons
bull no experimental evidence provided36
Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Current technological development paresthesia
bull Although paresthesias are assumed essential for pain relief when using conventional SCS (3233)
bull paresthesia can be uncomfortable (34)
bull Pain relief without paresthesia would expand the role of SCS
bull Burst and kilohertz-frequency stimulation arepotential solutions to the paresthesia problem
bull Currently multicenter randomized studies are under way in the USA
Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Current technological development
Position-adaptive SCS
bull SCS-induced paresthesia is dependent on body position39ndash41
bull more intensely in the supine position than in an upright position
bull variable thickness of the cerebrospinal fluid layer around the spinal cord
bull position of the spinal cord within the spinal canal exhibited considerable interindividual differences Holsheimer et al42
bull computer model they calculated the expected thresholdsbull devices are able to detect whether the patient is lying down or
standingbull automatic sensor-driven stimulation pt significantly more
satisfied than with manually stimulation45
SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

SCS for patients with FBSS is more effective the sooner an SCS system is implanted from the date of the previous failed surgery17
Importance of Timing With SCS in the Treatment of
FBSS
ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

ReferenceNumber of
PatientsFollow Up Results
North14 19 3 years ~50 reduced their medications
Van Buyten18 123 3 yearsAs a group reduced medication
use by gt50
Cameron19 766Up to 84
months45 reduced their medications
Taylor20 681 na 68 no longer needed analgesics
Reduction in Medication
Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Improvements in Daily Activities
ReferenceNumber of
PatientsFollow Up Results
Barolat9 41 1 yearAs a group significantly improved
function and mobility
North14 19 3 yearsAs a group improved in a range
of activities
ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

ReferenceNumber of
PatientsFollow Up Results
Van Buyten18 123 3 years 31 returned to work
Taylor20 1133 na 40 returned to work
Dario21 23 3 years 35 returned to work
Return to Work
Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Neuromodulation 2014 Aug17(6)515-50 Deer TR1
The appropriate use of neurostimulation of the spinal cord and peripheralnervous system for the treatment of chronic pain and ischemic diseases the
Neuromodulation Appropriateness Consensus Committee
bull International Neuromodulation Society (INS) evaluated evidence regarding the safety and efficacy of neurostimulationto treat chronic pain chronic critical limb ischemia and refractory angina and recommended appropriate clinical applications
bull literature reviews expert opinion clinical experience and individual research systematic reviews (1984 to 2013) and prospective and randomized controlled trials (2005 to 2013)
bull RCS support the efficacy of SCS in FBSS and CRPSbull International guidelines recommend spinal cord stimulation to
treat refractory anginabull studies of neurostimulation are needed for peripheral
neuropathic pain postamputation pain postherpetic neuralgia and other causes of nerve injury
Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Meacutelyagyi stimulaacutecioacute (DBS)
Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Első DBS a faacutejdalom kezeleacuteseacuteben
bull VPL (Mazars 1960 )
bull Capsula interna haacutetsoacute szaacuter (Adams 1974)
bull PAG (Reynolds 1969 )
bull CM-PF (Thoden 1979 Boivie-Meyerson 1982)
Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Acta Neurochir Suppl 200797(Pt 2)111-6Deep brain stimulation for neuropathic pain
Owen SL Green AL Nandi DD Bittar RG Wang S Aziz TZ
bull PVGPAG complex
bull PVG-thalamus gyuumlttes stimulaacutezoacuteja eredmeacutenyezi a legnagyobb faacutejdalomcsillapodaacutest
bull Kimenetel az etioloacutegiaacutetoacutel fuumlgg
bull Legjobb hataacutes fantom faacutejdalom arc-fej teruumlleti faacutejdalom eacutes anaesthesia dolorosa
bull post-stroke faacutejdalomra nem hataacutesos
Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Neurosurg Focus 2006 Dec 1521(6)E8Deep brain stimulation for the treatment of various chronic pain syndromes
Rasche D Rinaldi PC Young RF Tronnier VM
bull 56 pts with different forms of neuropathic and mixed nociceptiveneuropathic pain syndromes
bull follow-up 1 to 8 years mean 35 years bull Electrodes somatosensory thalamus and the
periventricular gray region bull The best long-term results chronic low-back and leg
pain (FBSS) neuropathic pain of peripheral origin (CRPS Type II)
bull Disappointing results central pain syndromes (spinal cord injury and poststroke pain)
Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Neurol Sci 2008 May29 Suppl 1S65-8Neuromodulation in treatment of refractory headaches
Franzini A Leone M Messina G Cordella R Marras C Bussone G Broggi G
bull cluster fejfaacutejaacutes trigeminus neuralgia
bull Deep Brain Stimulation (DBS)
bull Target Posterior Hypothalamus
Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Meacutelyagyi stimulaacutecioacute
kroacutenikus faacutejdalom
bull neospinothalamicus paacutelyaacutek vagy aacutetkapcsoloacute aacutellomaacutesai VPL IC PVG PAG VM PF septalis magok hypothalamus tegmentum
bull toumlbb koumlzpont egyuumlttes ingerleacutese (csak thalamus 58 PVGPAV eacutes thalamuscapsula interna egyuumltt 87)
bull nociceptiacutev faacutejdalom eredmeacutenyek jobbak mint deafferentaacutecioacutes tiacutepusnaacutel (63 vs 47)
bull leghateacutekonyabb FBSS (80)bull phantom faacutejdalom bull anaesthesia dolorosabull cluster fejfaacutejaacutes arcfaacutejdalom
bull Hataacutestalan central faacutejdalom (gerincvelő seacuteruumlleacutes poststroke faacutejdalom)
Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Neuromodulation 2014 Aug17(6)551-70 discussion 570 doi 101111ner12215
The appropriate use of neurostimulation stimulation of the intracranial and extracranial space and head for chronic pain Neuromodulation
Appropriateness Consensus CommitteeDeer TR1 Mekhail N Petersen E Krames E Staats P Pope J Saweris Y Lad SP Diwan S Falowski S Feler C
Slavin K Narouze S Merabet L Buvanendran A Fregni F Wellington J Levy RM NeuromodulationAppropriateness Consensus Committee
bull evidence supports extracranial stimulation for facial pain migraine and scalp pain
bull evidence is limited for intracranial neuromodulation
bull High cervical spinal cord stimulation is an evolving option for facial pain
bull Intracranial neurostimulation for pain should be seen as investigational
bull extracranial nerve stimulation should be considered in the algorithmic treatment of migraine and other disorders of the head
Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Motor cortex stimulaacutecioacute
Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Motoros cortex stimulaacutecioacute (MCS)
bull Centraacutelis deafferentaacutecioacutes faacutejdalom neuropathiaacutes arcfaacutejdalom nem reagaacutelt a klasszikus stimulaacutecioacutes technikaacutekra a thalamusban
bull Tsubokawa 1991 centraacutelis laesio (thalamus faacutejdalom) abnormaacutelis neuronaacutelis aktivitaacutes a thalamusban ami a MCS-val csillapodik
MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

MCS indikaacutecioacutek
bull deafferentaacutecioacutes arcfaacutejdalom
bull centraacutelis faacutejdalom
DE
bull teljes deafferentaacutecioacutes arcfaacutejdalom teljes beacutenulaacutessal suacutelyos motoros deficittel jaacuteroacute faacutejdalom rossz prognosztikai faktor
Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Hataacutesmechanizmus (MCS)
bull rCBF vaacuteltozaacutes Koumlzeacutepvonali thalamus magok anterior gyrus cinguli agytoumlrzs felső reacutesze(Garcia-Larrea 1999)
bull A pyramis paacutelya direkt hataacutest gyakorol a gvelő haacutetsoacute szarvra (Coulter 1974)
bull Ingerleacutes a somatotopiaacutenak megfelelőteruumlleten hateacutekony (Nguyen 1999)
MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

MCS felteacutetelezhető hataacutesmechanizmusai
bull A nem nociteptiacutev szenzoros inputok nociteptiacutev rendszer foumlloumltti megerősiacuteteacutese reacuteveacuten fejti ki hataacutesaacutet a thalamus szintjeacuten
bull Csoumlkkenti a faacutejdalom emocionaacutelis komponenseit az anterior cingulaacuteris cortex eacutes az anterior inzula aktivaacutelaacutesa reacuteveacuten
J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

J Neurosurg 2015 Aug 141-11 [Epub ahead of print]Motor cortex stimulation and neuropathic pain how does motor cortex stimulation affect pain-signaling pathways
Kim J123 Ryu SB4 Lee SE56 Shin J12 Jung HH2 Kim SJ567 Kim KH4 Chang JW12
bull MCS modulated ascending and descending pain pathways
bull It regulated neuropathic pain by affecting the striatum periaqueductal gray cerebellum and thalamic area which are thought to regulate the descending pathway
bull MCS also suppress activation of the VPL which is part of the ascending pathway
J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

J Neurol Surg A Cent Eur Neurosurg 2015 Sep 9 [Epub ahead of print]
Treatment of Central Deafferentation and Trigeminal Neuropathic Pain by Motor CortexStimulation Report of a Series of 20 Patients
Kolodziej MA1 Hellwig D2 Nimsky C3 Benes L3
bull Conclusions MCS is an effective treatment modality for central neuropathic pain and trigeminal pain with low morbidity and mortality
bull Future studies are necessary to evaluate and optimize this treatment option in more detail
Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Can J Neurol Sci 2015 Sep 11-9 [Epub ahead of print]
Motor Cortex Stimulation for Neuropathic Pain A Randomized Cross-over Trial
Radic JA1 Beauprie I2 Chiasson P1 Kiss ZH3 Brownstone RM1
bull CONCLUSIONS
bull We failed to show that MCS is an effective treatment for refractory upper extremity neuropathic pain
bull We suggest that a healthy degree of skepticism is warranted when considering this invasive therapy for upper extremity pain syndromes
Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Peripheral Nerve Field Stimulation
Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Dorsal Root Ganglion Electrical Stimulation
Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Dorsal Root Ganglion Electrical Stimulation
bull DRG integral to the development of both nociceptive and neuropathic pain (53)
bull The development of neuropathic pain is complex and involves different cell types that include DRG cell bodies satellite glial cells that wrap and surround the pseudo-unipolar DRG somata glial cells astrocytes and Schwanncells the immune system and neuronal pathways (55)
bull A massive spontaneous discharge within large axotomizedA-neurons within the DRG occurs after cutting spinalnerves distal to the DRG (56) Sukhotinsky et al (56) support the hypothesis that ldquoectopic firing in DRG A-neurons induces central sensitizationrdquo (57) and clinicalallodynia
Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Current technological development
Dorsal root ganglion stimulation
bull electrode is placed adjacent to the spinal ganglion
bull paresthesia within a single dermatome
bull energy consumption significantly less76
bull pain relief strongest in the feet and weakest in the low back77
bull in monoradicular pain
bull limited number of dermatomes
Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Neuromodulation 2014 Oct17(7)678-85 discussion 685 doi 101111ner12186 Epub2014 May 6
International neuromodulation society critical assessment guidelinereview of implantable neurostimulation devices
Deer TR1 Thomson S Pope JE Russo M Luscombe F Levy R
bull to review the relevant guideline statements for implantable neurostimulation therapies to treat chronic pain and to identify guideline gaps and future directions for recommendation platforms
bull A systematic literature search through EMBASE Medline Cochrane data base
bull Based on these deficiencies the International Neuromodulation Society recommended the creation of a consensus conference to examine the appropriate use of neurostimulation for pain and ischemic disease
SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

SAFETY OF NEUROSTIMULATIONCompared With High-Dose Opioids
bull high-dose long-term opioid side effects hormonal and immune system dysfunction depression weight gain tolerance opioid-induced hyperalgesia (OIH) and the potential for dependence abuse and addiction (141ndash 145)
bull overdose deaths (146147) with opioid 74 (14800 of 20044) in 2008
bull oral opioids long-term (more than six months) efficacyare lacking (148149)
bull opioid therapy questionable in neuropathic pain(150151)
Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Compared with Conservative Medical Management
bull PROCESS study (161) comparing SCS withCMMin a randomized and controlled manner SCS is superior to CMM
bull Literature reviews in 2011 and 2013 of the safety appropriateness fiscal neutrality and effectiveness (SAFE) of SCS suggest that it be considered before submitting patients to long-term opioid therapy for chronic pain from FBSS and CRPS (163164)
Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Compared With Spine Surgery
bull North (127) randomized 60 FBSS patients toeither SCS or repeated lumbosacral spine surgery with an average follow-up of threeyears
bull SCS is more effective than reoperation for radicular pain after lumbosacral spinesurgery
Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Failure of Conservative Medical ManagementNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull NACC recommends
bull neuromodulation should be used in patients who fail to have acceptable relief or have unmanageable side effects with conservative treatment
bull evidence that SCS should be used beforeanother back surgery for FBSS (127) and
bull before starting systemic long-acting opioids(163)
Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Contraindications
bull active uncontrolled psychiatric disorder
bull infection immunosuppression and anticoagulant or antiplatelet therapy that cannot be suspended (191)
bull Previously failed trial but kilohertz-frequency SCS burst SCS DRG stimulation suggests that there is not necessarily a correlation between a failed trial with conventional SCS and future success (20ndash2227192)
bull NACC recommends consider using new technologies who have failed trials of conventional SCS
Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Keacutemiai neuromodulaacutecioacute -gyoacutegyszeradagolaacutes helye
bull intraspinaacutelis (IS)
bull intracerebroventricularis (ICVDDS)
IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

IDA DDS indikaacutecioacutek
bull diffuacutez daganatos faacutejdalom
bull somaticus visceraacutelis faacutejdalom (daganat chr pancretitis)
bull osteoporosis
bull nociceptiacutev faacutejdalom
bull multiplex faacutejdalom (trunkaacutelisaxiaacutelis)
Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Pain Physician 2011 May-Jun14(3)219-48Intrathecal therapy for cancer and non-cancer pain
Hayek SM1 Deer TR Pope JE Panchal SJ Patel VB
bull Literature search through EMBASE Medline Cochrane databases and systematic reviews as well as peer-reviewed non-indexed journals from 1980 to December 2010
bull CONCLUSION
bull evidence for cancer-related pain is moderate
bull evidence limited to moderate from non-randomized studies for non-cancer related pain
Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Konkluacutezioacute
PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

PNS (PNfS) for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull For head and neck the committee said that when possible extracranial stimulation should be an earlier option in the treatment algorithmbdquo
bull CE mark approved in Europe
-occipital neuralgia
-chronic migraine
bull Medtronic CE Mark
-Chronic Back Pain
SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

SCS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull approved by the FDA for-failed back surgery syndrome -complex regional pain syndrome -radiculopathy (traumatic neuropathies diabetic neuropathy postherpetic neuralgia)
bull In Europe CE mark for-refractory angina pectoris-peripheral limb ischemia
DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

DBS for painNeuromodulation 2014 Aug17(6)515-50 Deer TR1
bull DBS is limited by its inherent invasiveness and risks
bull for certain painful conditions including facial pain due to damaged trigeminal nerves
bull may not be the best treatment for painbull has not been tested for this in randomized
clinical trials
MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

MCS for pain Surg Neurol Int 2012 3(Suppl 4) S290ndashS311
bull facial chronic neuropathic pain
bull safe and efficacious when previous managements have failed
bull most successful for
bull trigeminal neuropathicdeafferentation pain
bull central poststroke pain
bull however there is still lack of strong evidence (larger randomized controlled multicentrestudies)
Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Neuromodulaacutecioacuteneuropaacutetiaacutes faacutejdalom konkluacutezioacutek
bull SCS bdquoon- labelrdquo FBSS CRPS (level B) angina PVD
bull PNS bdquoon- labelrdquo ndash migreacuten occipitaacutelis neuralgia (fej-nyak faacutejdalom)ndash LBP (dereacutekfaacutejdalom)
bull IDA bdquoon -labelrdquo diffuacutez multiplex faacutejdalmak főleg daganatos
bull DBS bdquooff labelrdquo arc-fej faacutejdalom cluster bull MCS bdquooff labelrdquo centraacutelis post-stroke eacutes
deafferentaacutecioacutes arcfaacutejdalom (level C)
SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

SCS indikaacutecioacutek VISacralis ideg stimlaacutecioacute (SNS)
bull Alo 1999 Chancellor Chartier-Kastler 2000 Windaele 2000
Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Tined Leads Models
Anchoring with Tines
S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

S 1
S 2
S 3
S 4
Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Sacralis ideg stimlaacutecioacute (SNS)indikaacutecioacutek
bull Urologiai betegseacutegek (suumlrgősseacutegi-incontinenciaOAB retencioacute)
bull Szeacutekletszabaacutelyozaacutesi zavarok
bull Perineaacutelis genitaacutelis rectaacutelis pelvis faacutejdalom (pl interstitial cystitis) csak ha sphincterzavarral kombinaacuteloacutedik
Koumlszoumlnoumlm a figyelmet

Koumlszoumlnoumlm a figyelmet