Embed Size (px)
Citation preview
Bukowina Tatrzańska 4-6 grudnia 2014
Opryszczkowate zapalenie skoacutery czy jest to
schorzenie zasadniczo skoacuterne
Marian Dmochowski Kierownik Pracownia Autoimmunizacyjnych Dermatoz Pęcherzowych Katedra i Klinika Dermatologii UM w Poznaniu wwwdmochowskicompl mkdmochowskigmailcom
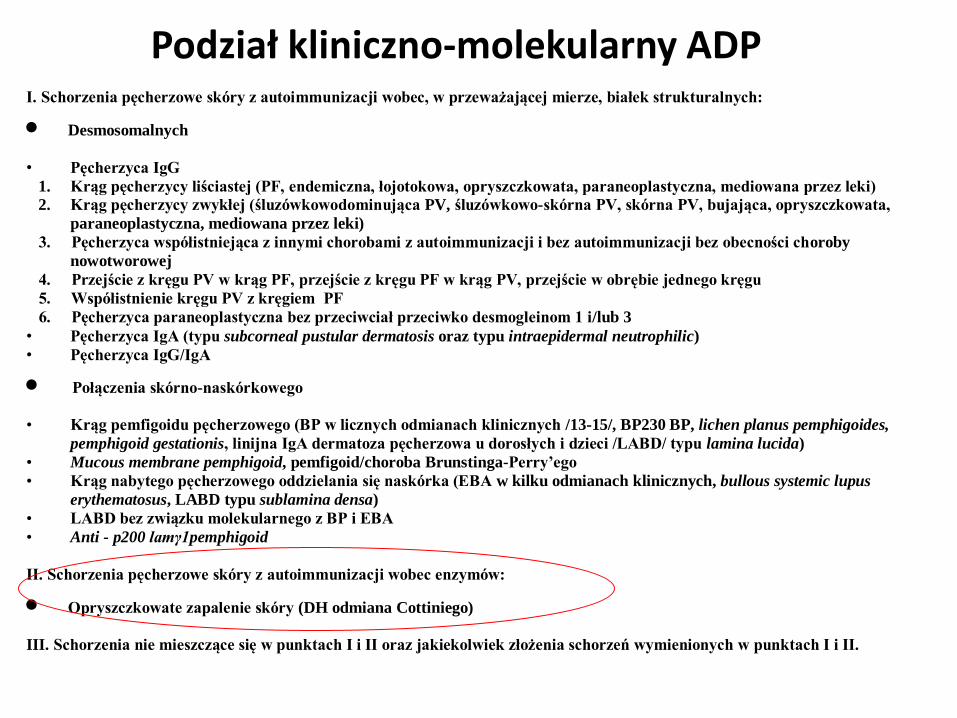
Podział kliniczno-molekularny ADP I Schorzenia pęcherzowe skoacutery z autoimmunizacji wobec w przeważającej mierze białek strukturalnych
Desmosomalnych
bull Pęcherzyca IgG
1 Krąg pęcherzycy liściastej (PF endemiczna łojotokowa opryszczkowata paraneoplastyczna mediowana przez leki)
2 Krąg pęcherzycy zwykłej (śluzoacutewkowodominująca PV śluzoacutewkowo-skoacuterna PV skoacuterna PV bujająca opryszczkowata
paraneoplastyczna mediowana przez leki)
3 Pęcherzyca wspoacutełistniejąca z innymi chorobami z autoimmunizacji i bez autoimmunizacji bez obecności choroby
nowotworowej
4 Przejście z kręgu PV w krąg PF przejście z kręgu PF w krąg PV przejście w obrębie jednego kręgu
5 Wspoacutełistnienie kręgu PV z kręgiem PF
6 Pęcherzyca paraneoplastyczna bez przeciwciał przeciwko desmogleinom 1 ilub 3 bull Pęcherzyca IgA (typu subcorneal pustular dermatosis oraz typu intraepidermal neutrophilic)
bull Pęcherzyca IgGIgA
Połączenia skoacuterno-naskoacuterkowego
bull Krąg pemfigoidu pęcherzowego (BP w licznych odmianach klinicznych 13-15 BP230 BP lichen planus pemphigoides
pemphigoid gestationis linijna IgA dermatoza pęcherzowa u dorosłych i dzieci LABD typu lamina lucida)
bull Mucous membrane pemphigoid pemfigoidchoroba Brunstinga-Perryrsquoego
bull Krąg nabytego pęcherzowego oddzielania się naskoacuterka (EBA w kilku odmianach klinicznych bullous systemic lupus
erythematosus LABD typu sublamina densa)
bull LABD bez związku molekularnego z BP i EBA
bull Anti - p200 lamγ1pemphigoid
II Schorzenia pęcherzowe skoacutery z autoimmunizacji wobec enzymoacutew
Opryszczkowate zapalenie skoacutery (DH odmiana Cottiniego)
III Schorzenia nie mieszczące się w punktach I i II oraz jakiekolwiek złożenia schorzeń wymienionych w punktach I i II
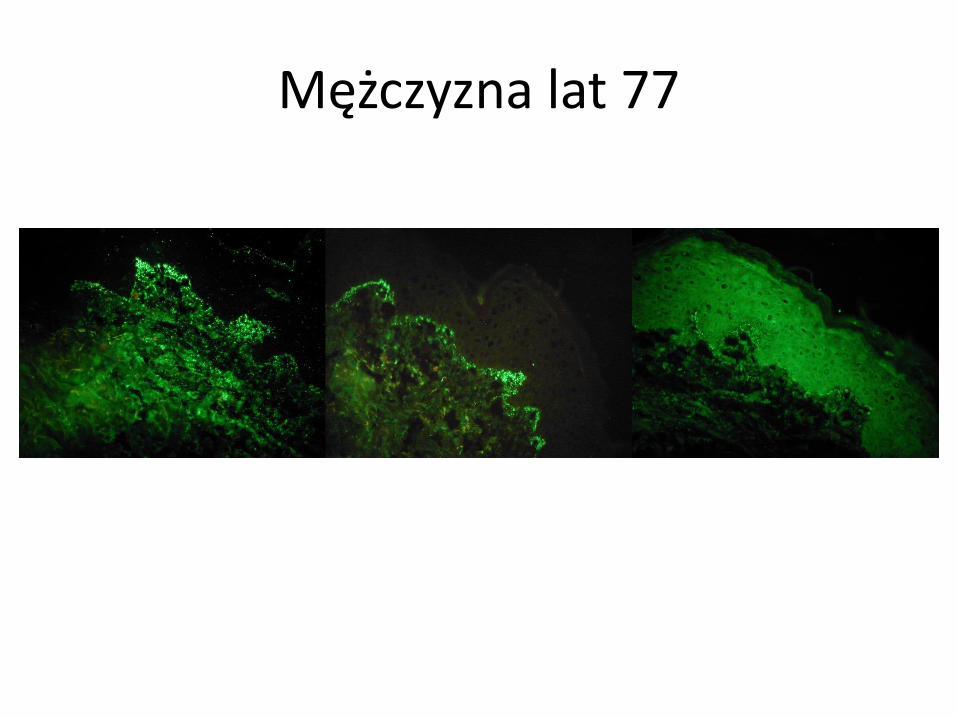
Mężczyzna lat 77
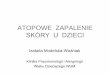
Oral Surg Oral Med Oral Pathol 1982 Jul54(1)22-5
Dermatitis herpetiformis IgA deposits in gingiva buccal
mucosa and skin
Nisengard RJ Chorzelski T Maciejowska E Kryst L
Abstract
Fourteen patients who had dermatitis herpetiformis of the skin with no
gingival lesions were studied In each patient biopsy specimens of
normal gingiva buccal mucosa and perilesional skin were examined
for IgA and IgG deposits Depending on the method of handling
biopsy specimens for immunofluorescence IgA deposits were
detected in 21 to 25 percent of gingival specimens 27 to 46 percent
of buccal mucosal specimens and 64 to 76 percent of skin
specimens The occurrence of IgA deposits in the gingival papillae a
site where lesions of DH have not been reported in the past or
observed in this study suggests that these IgA deposits alone may
not play a primary role in the pathogenesis of this disease Similar
immunofluorescent findings of IgA deposits were observed in both
quick-frozen biopsy specimens and those placed in holding solution
indicating the suitability of the holding solution for transporting
suggested DH biopsy material
PMID 6750497 [PubMed - indexed for MEDLINE]
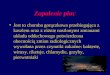
We hypothesize that the IgA class
anti-TG3 Abs are directly
responsible
for the immune deposits and that
the TG3 is from human epidermis
as this is its only source in our
model
Epidermal transglutaminase
Patients with DH had elevated levels of IgA anti-TG3 (Fig 2) Twenty-three of 44 (52) had IgA anti-TG3 levels
gt 18 units
Wyniki Zaledwie u 8 spośroacuted 21
(38) chorych na DH stwierdzono że
wyniki badań TG3 IF oraz badań IgA
TG3 ELISA były zbieżne (wyniki badań
obiema
metodami pozytywne oraz wyniki
badań obiema metodami negatywne)
Wnioski Wyniki niniejszego
doniesienia zdają się sugerować że u
chorych na DH zjawiska zależne od
TG3 na poziomie krwiobiegu i na
poziomie skoacuternym
nie są jeżeli chodzi o patogenezę tej
choroby powiązane w znaczącym
stopniu
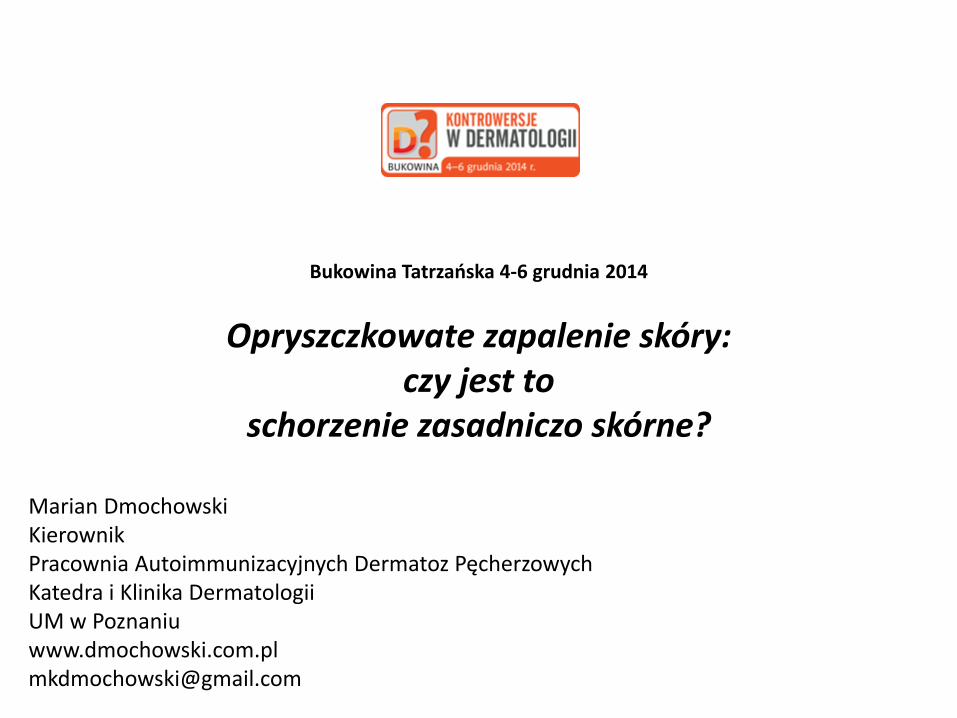
Cutaneous expression of neutrophil elastase in relation
to IgA antibodies to nonapeptides of gliadin and
tissue transglutaminase in dermatitis
herpetiformis
Results
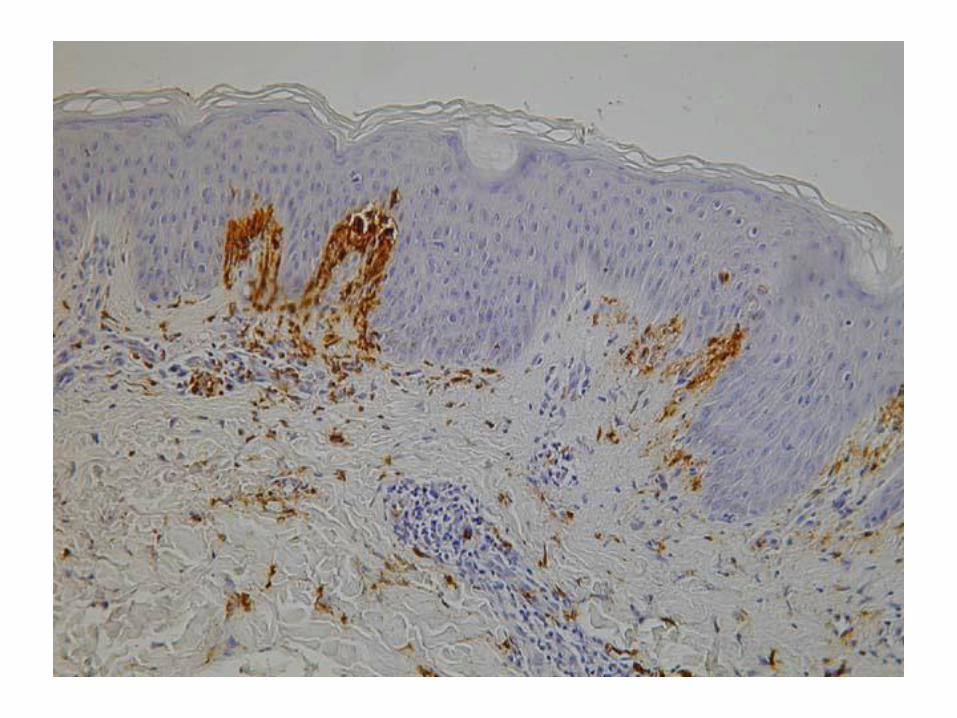
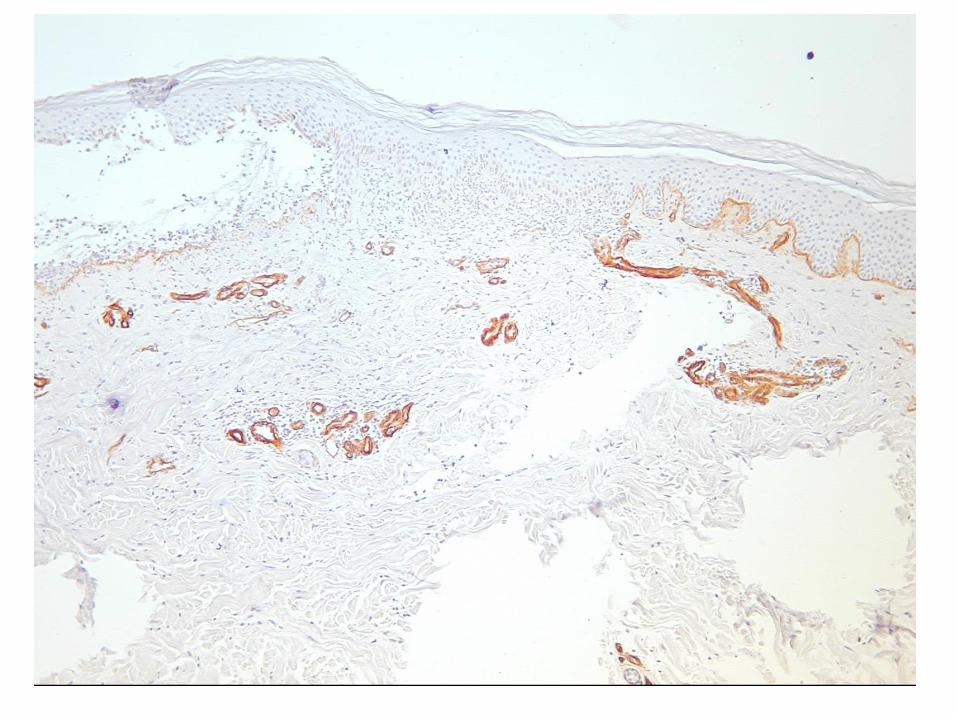
NE (top left) deposits in immunohistochemistry in
lesional skin in a male patient with DH
(immunoperoxidase staining on paraffin embedded
sections original magnification x200)
Intensity of NE (bottom left) deposits processed
with digital microscopic image analysis
superimposed on NE deposits
in immunohistochemistry in lesional skin in
this patient
Intensity of NE (top right) deposits processed with
digital microscopic image analysis in lesional skin in
this patient
Conclusions
bull Thus it seems that the production of IgA npG takes place in a coordinated way with the production of IgA tTG when patients show cutaneous lesions of DH
bull Nevertheless it is hypothesized that IgA npG and IgA tTG regardless of the issue of their diagnostic significance have lesser importance as far as cutaneous pathology of human DH mediated by DEJ-degrading NE released from IgA autoimmunity-activated neutrophils is concerned
Consistently with the autoimmune
origin of DH functional classification
of the differentially expressed genes
(DEGs) indicates a B- and T-cell
immune response (LAG3 TRAF5
DPP4 and NT5E) In addition gene
modulation provides evidence for a
local inflammatory response (IL8
PTGFR FSTL1 IFI16 BDKRD2
and NAMPT) with concomitant
leukocyte recruitment (CCL5
ENPP2) endothelial cell activation
and neutrophil extravasation (SELL
SELE) DEGs also indicate
overproduction of matrix proteases
(MMP9 ADAM9 and ADAM19) and
proteolytic enzymes (CTSG ELA2
CPA3 TPSB2 and CMA1) that may
contribute to epidermal splitting and
blister formation
In conclusion our data add DH
plaque psoriasis and
psoriatic arthritis to the growing
list of disorders associated
with Ig deregulation where the
enhancer HS12-A may be
involved
The incubation with Ni-Ti heat-
activated (T3) or Ni-Ti super-elastic
(T4) and with Ni-Cr-Co (T2) alloys
produced respectively 25-fold and 8-
fold increases in IL-6 release
compared with control cultures
Transglutaminase activity was
significantly increased in cells
exposed to T3 and T4 alloys (about
170 of control p lt 005) where it
was mainly localized close to inner
part of cell membrane The exposure
to T3 and T4 specimens significantly
up-regulated also tTG expression
compared with control cultures
These data first show an association
between IL-6 release and tissue
transglutaminase increases
suggesting that TGase-mediated
reactions may play a major role in
periodontal inflammation
pp 178-9
DH patomechanizm
Uważam że należy postrzegać DH jako chorobę skoacuterną z drugorzędnym udziałem patologii jelitowej
Sądzę że w skoacuternej patogenezie tej dermatozy wspoacutełgrają wzajemnie zapętlone zjawiska autoimmunizacji zależne od kluczowego autoantygenu ndash enzymu transglutaminazy naskoacuterkowej (eTG) przemieszczonej być może w wyniku mikrourazoacutew i drapania do skoacutery właściwej w bliskości połączenia skoacuterno-naskoacuterkowego (dermal-epidermal junction DEJ) z wyższych warstw naskoacuterka gdzie ma ona znaczenie fizjologiczne jako bdquoklej biologicznyrdquo (jeden z elementoacutew bdquobariery naskoacuterkowejrdquobdquokoperty rogowejrdquo) oraz (auto)zapalenia zależnego od uczynnionych neutrofiloacutew uwalniających elastazę neutrofiloacutew (NE) trawiącą DEJ z wytworzeniem rozwarstwienia w przestrzeni lamina lucida
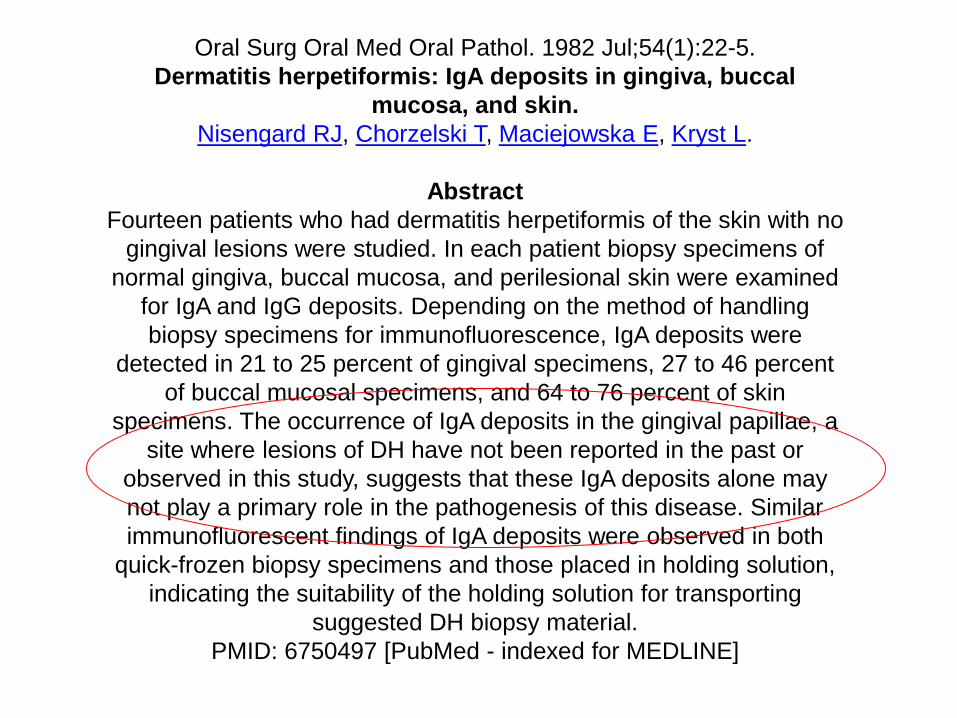
DH postępowanie diagnostyczne
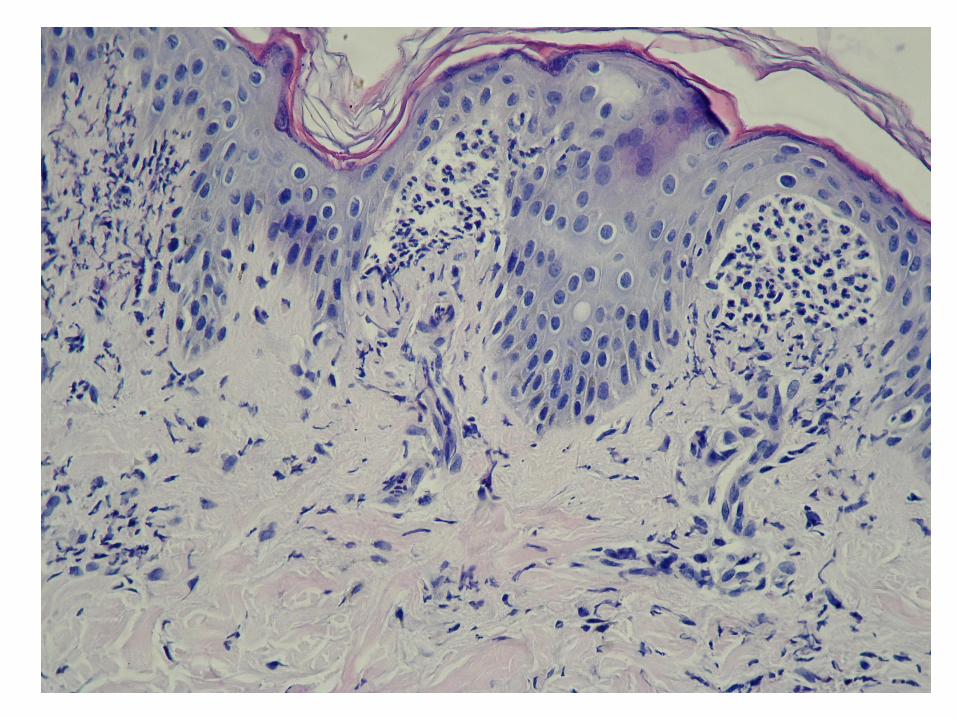
Standardem diagnostyki roacuteżnicowej DH powinno być postępowanie troacutejskładnikowe oparte o badanie kliniczne (co i gdzie)(stereotypowym chorym będzie młodzieniec lub młody mężczyzna) bezpośrednie badanie immunofluorescencyjne (DIF)skoacutery klinicznie niezmienionej z otoczenia wykwitoacutew analogicznie do pozostałych autoimmunizacyjnych dermatoz pęcherzowych (ujawnia definiujące to schorzenie złogi IgA w co najmniej 7 wzorach) oraz oznaczenie surowiczych przeciwciał IgA techniką ELISA z jednym substratem do wyboru z zakresu transglutaminaza tkankowa (tTG) eTG nonapeptydy gliadyny (npG) neoepitopy gliadyna-tTG (neo-tTG) Owo postępowanie można uzupełnić o badanie histologiczne H+E wycinka ze skoacutery wykwitowej i badanie haplotypu HLA DQ2DQ8 u chorych z niejednoznacznym obrazem kliniczno-pracownianym
DH postępowanie lecznicze
Standardem terapeutycznym w DH czyli generalnie postępowaniem terapeutycznym z wyboru powinno natomiast być postępowanie dwuskładnikowe czyli powiązanie leczenia farmakologicznego kluczowym dapsonem i dietetycznego dietą bezglutenową w indywidualizowanych kombinacjach W postępowaniu leczniczym trzeba też uwzględnić całość problemoacutew zdrowotnych chorego
ACTA DERMATO-VENEREOLOGICA REVIEWERacuteS COMMENTS TO THE AUTHOR(S) Re Manuscript 114366 Authors Pasternack et al Title Quality of life and gastrointestinal symptoms in long-term g The authors analysed the HRQoL in DH patients on gluten free diet The topic is interesting however the study design is questionable First af all dermatitis herpetiformis is not a cutaneous manifestation of coeliac disease but it is rather a cutaneous disease associated with coeliac disease Furthermore the healthy group is poorly characterized (eg concomitant diseases are not mentioned at all eg Diabetes arterial hypertension) No comparison was performed regarding the age and gender distribution between DH patients and controls As there are differences within the DH patients regarding males and females a very low proportion of men in control group is an important bias as it seems that gender may be relevant cofactor In addition I would rather expect comparison between DH menhealthy men and DH womenhealthy women rather than between DH menDH women as the HRQOL in DH patients has been shown to be similar to controls The authors claimed that having ongoing skin symptoms at the time of the study had no influence on GSRS PGWB or SF-36 scores and the data are not shown In my opinion it is very probable that lack of significance was related to very small number of patients in the group of active skin lesions I would also expect from the authors to provide the information about concomitant gastrointestinal symptoms at the time of DH diagnosis It is probable that many of these patients never had clinically relevant symptoms of coeliac disease and thus GSRS would rather assess the effect of gluten-free diet on gastrointestinal symptoms instead of the relevance of coeliac disease symptomatology
Opryszczkowate zapalenie skoacutery jest
schorzeniem skoacuternym
bull nozologia DH jest zwodnicza dla wspoacutełczesnej społeczności
zwłaszcza niedermatologicznej
(opryszczkopodobne zapalenie skoacutery)
bull kontinuum autoimmunizacji i (auto)zapalenia
bull kluczowymi w skoacuternej patologii jawią się eTG i neutrofil
(uchwycenie zjawisk skoacuternych jak najbardziej DH-specyficznych)
bull DH to zapewne choroba skoacuterna z towarzyszącą nadwrażliwością na gluten
nieporozumienia
bull dapson na import docelowy
bull okolica łokciowa
bull pośladek jako miejsce wykonania DIFf
bull
foto Zbyszek KaczmarekGazeta Polska
Podział kliniczno-molekularny ADP I Schorzenia pęcherzowe skoacutery z autoimmunizacji wobec w przeważającej mierze białek strukturalnych
Desmosomalnych
bull Pęcherzyca IgG
1 Krąg pęcherzycy liściastej (PF endemiczna łojotokowa opryszczkowata paraneoplastyczna mediowana przez leki)
2 Krąg pęcherzycy zwykłej (śluzoacutewkowodominująca PV śluzoacutewkowo-skoacuterna PV skoacuterna PV bujająca opryszczkowata
paraneoplastyczna mediowana przez leki)
3 Pęcherzyca wspoacutełistniejąca z innymi chorobami z autoimmunizacji i bez autoimmunizacji bez obecności choroby
nowotworowej
4 Przejście z kręgu PV w krąg PF przejście z kręgu PF w krąg PV przejście w obrębie jednego kręgu
5 Wspoacutełistnienie kręgu PV z kręgiem PF
6 Pęcherzyca paraneoplastyczna bez przeciwciał przeciwko desmogleinom 1 ilub 3 bull Pęcherzyca IgA (typu subcorneal pustular dermatosis oraz typu intraepidermal neutrophilic)
bull Pęcherzyca IgGIgA
Połączenia skoacuterno-naskoacuterkowego
bull Krąg pemfigoidu pęcherzowego (BP w licznych odmianach klinicznych 13-15 BP230 BP lichen planus pemphigoides
pemphigoid gestationis linijna IgA dermatoza pęcherzowa u dorosłych i dzieci LABD typu lamina lucida)
bull Mucous membrane pemphigoid pemfigoidchoroba Brunstinga-Perryrsquoego
bull Krąg nabytego pęcherzowego oddzielania się naskoacuterka (EBA w kilku odmianach klinicznych bullous systemic lupus
erythematosus LABD typu sublamina densa)
bull LABD bez związku molekularnego z BP i EBA
bull Anti - p200 lamγ1pemphigoid
II Schorzenia pęcherzowe skoacutery z autoimmunizacji wobec enzymoacutew
Opryszczkowate zapalenie skoacutery (DH odmiana Cottiniego)
III Schorzenia nie mieszczące się w punktach I i II oraz jakiekolwiek złożenia schorzeń wymienionych w punktach I i II
Mężczyzna lat 77
Oral Surg Oral Med Oral Pathol 1982 Jul54(1)22-5
Dermatitis herpetiformis IgA deposits in gingiva buccal
mucosa and skin
Nisengard RJ Chorzelski T Maciejowska E Kryst L
Abstract
Fourteen patients who had dermatitis herpetiformis of the skin with no
gingival lesions were studied In each patient biopsy specimens of
normal gingiva buccal mucosa and perilesional skin were examined
for IgA and IgG deposits Depending on the method of handling
biopsy specimens for immunofluorescence IgA deposits were
detected in 21 to 25 percent of gingival specimens 27 to 46 percent
of buccal mucosal specimens and 64 to 76 percent of skin
specimens The occurrence of IgA deposits in the gingival papillae a
site where lesions of DH have not been reported in the past or
observed in this study suggests that these IgA deposits alone may
not play a primary role in the pathogenesis of this disease Similar
immunofluorescent findings of IgA deposits were observed in both
quick-frozen biopsy specimens and those placed in holding solution
indicating the suitability of the holding solution for transporting
suggested DH biopsy material
PMID 6750497 [PubMed - indexed for MEDLINE]
We hypothesize that the IgA class
anti-TG3 Abs are directly
responsible
for the immune deposits and that
the TG3 is from human epidermis
as this is its only source in our
model
Epidermal transglutaminase
Patients with DH had elevated levels of IgA anti-TG3 (Fig 2) Twenty-three of 44 (52) had IgA anti-TG3 levels
gt 18 units
Wyniki Zaledwie u 8 spośroacuted 21
(38) chorych na DH stwierdzono że
wyniki badań TG3 IF oraz badań IgA
TG3 ELISA były zbieżne (wyniki badań
obiema
metodami pozytywne oraz wyniki
badań obiema metodami negatywne)
Wnioski Wyniki niniejszego
doniesienia zdają się sugerować że u
chorych na DH zjawiska zależne od
TG3 na poziomie krwiobiegu i na
poziomie skoacuternym
nie są jeżeli chodzi o patogenezę tej
choroby powiązane w znaczącym
stopniu
Cutaneous expression of neutrophil elastase in relation
to IgA antibodies to nonapeptides of gliadin and
tissue transglutaminase in dermatitis
herpetiformis
Results
NE (top left) deposits in immunohistochemistry in
lesional skin in a male patient with DH
(immunoperoxidase staining on paraffin embedded
sections original magnification x200)
Intensity of NE (bottom left) deposits processed
with digital microscopic image analysis
superimposed on NE deposits
in immunohistochemistry in lesional skin in
this patient
Intensity of NE (top right) deposits processed with
digital microscopic image analysis in lesional skin in
this patient
Conclusions
bull Thus it seems that the production of IgA npG takes place in a coordinated way with the production of IgA tTG when patients show cutaneous lesions of DH
bull Nevertheless it is hypothesized that IgA npG and IgA tTG regardless of the issue of their diagnostic significance have lesser importance as far as cutaneous pathology of human DH mediated by DEJ-degrading NE released from IgA autoimmunity-activated neutrophils is concerned
Consistently with the autoimmune
origin of DH functional classification
of the differentially expressed genes
(DEGs) indicates a B- and T-cell
immune response (LAG3 TRAF5
DPP4 and NT5E) In addition gene
modulation provides evidence for a
local inflammatory response (IL8
PTGFR FSTL1 IFI16 BDKRD2
and NAMPT) with concomitant
leukocyte recruitment (CCL5
ENPP2) endothelial cell activation
and neutrophil extravasation (SELL
SELE) DEGs also indicate
overproduction of matrix proteases
(MMP9 ADAM9 and ADAM19) and
proteolytic enzymes (CTSG ELA2
CPA3 TPSB2 and CMA1) that may
contribute to epidermal splitting and
blister formation
In conclusion our data add DH
plaque psoriasis and
psoriatic arthritis to the growing
list of disorders associated
with Ig deregulation where the
enhancer HS12-A may be
involved
The incubation with Ni-Ti heat-
activated (T3) or Ni-Ti super-elastic
(T4) and with Ni-Cr-Co (T2) alloys
produced respectively 25-fold and 8-
fold increases in IL-6 release
compared with control cultures
Transglutaminase activity was
significantly increased in cells
exposed to T3 and T4 alloys (about
170 of control p lt 005) where it
was mainly localized close to inner
part of cell membrane The exposure
to T3 and T4 specimens significantly
up-regulated also tTG expression
compared with control cultures
These data first show an association
between IL-6 release and tissue
transglutaminase increases
suggesting that TGase-mediated
reactions may play a major role in
periodontal inflammation
pp 178-9
DH patomechanizm
Uważam że należy postrzegać DH jako chorobę skoacuterną z drugorzędnym udziałem patologii jelitowej
Sądzę że w skoacuternej patogenezie tej dermatozy wspoacutełgrają wzajemnie zapętlone zjawiska autoimmunizacji zależne od kluczowego autoantygenu ndash enzymu transglutaminazy naskoacuterkowej (eTG) przemieszczonej być może w wyniku mikrourazoacutew i drapania do skoacutery właściwej w bliskości połączenia skoacuterno-naskoacuterkowego (dermal-epidermal junction DEJ) z wyższych warstw naskoacuterka gdzie ma ona znaczenie fizjologiczne jako bdquoklej biologicznyrdquo (jeden z elementoacutew bdquobariery naskoacuterkowejrdquobdquokoperty rogowejrdquo) oraz (auto)zapalenia zależnego od uczynnionych neutrofiloacutew uwalniających elastazę neutrofiloacutew (NE) trawiącą DEJ z wytworzeniem rozwarstwienia w przestrzeni lamina lucida
DH postępowanie diagnostyczne
Standardem diagnostyki roacuteżnicowej DH powinno być postępowanie troacutejskładnikowe oparte o badanie kliniczne (co i gdzie)(stereotypowym chorym będzie młodzieniec lub młody mężczyzna) bezpośrednie badanie immunofluorescencyjne (DIF)skoacutery klinicznie niezmienionej z otoczenia wykwitoacutew analogicznie do pozostałych autoimmunizacyjnych dermatoz pęcherzowych (ujawnia definiujące to schorzenie złogi IgA w co najmniej 7 wzorach) oraz oznaczenie surowiczych przeciwciał IgA techniką ELISA z jednym substratem do wyboru z zakresu transglutaminaza tkankowa (tTG) eTG nonapeptydy gliadyny (npG) neoepitopy gliadyna-tTG (neo-tTG) Owo postępowanie można uzupełnić o badanie histologiczne H+E wycinka ze skoacutery wykwitowej i badanie haplotypu HLA DQ2DQ8 u chorych z niejednoznacznym obrazem kliniczno-pracownianym
DH postępowanie lecznicze
Standardem terapeutycznym w DH czyli generalnie postępowaniem terapeutycznym z wyboru powinno natomiast być postępowanie dwuskładnikowe czyli powiązanie leczenia farmakologicznego kluczowym dapsonem i dietetycznego dietą bezglutenową w indywidualizowanych kombinacjach W postępowaniu leczniczym trzeba też uwzględnić całość problemoacutew zdrowotnych chorego
ACTA DERMATO-VENEREOLOGICA REVIEWERacuteS COMMENTS TO THE AUTHOR(S) Re Manuscript 114366 Authors Pasternack et al Title Quality of life and gastrointestinal symptoms in long-term g The authors analysed the HRQoL in DH patients on gluten free diet The topic is interesting however the study design is questionable First af all dermatitis herpetiformis is not a cutaneous manifestation of coeliac disease but it is rather a cutaneous disease associated with coeliac disease Furthermore the healthy group is poorly characterized (eg concomitant diseases are not mentioned at all eg Diabetes arterial hypertension) No comparison was performed regarding the age and gender distribution between DH patients and controls As there are differences within the DH patients regarding males and females a very low proportion of men in control group is an important bias as it seems that gender may be relevant cofactor In addition I would rather expect comparison between DH menhealthy men and DH womenhealthy women rather than between DH menDH women as the HRQOL in DH patients has been shown to be similar to controls The authors claimed that having ongoing skin symptoms at the time of the study had no influence on GSRS PGWB or SF-36 scores and the data are not shown In my opinion it is very probable that lack of significance was related to very small number of patients in the group of active skin lesions I would also expect from the authors to provide the information about concomitant gastrointestinal symptoms at the time of DH diagnosis It is probable that many of these patients never had clinically relevant symptoms of coeliac disease and thus GSRS would rather assess the effect of gluten-free diet on gastrointestinal symptoms instead of the relevance of coeliac disease symptomatology
Opryszczkowate zapalenie skoacutery jest
schorzeniem skoacuternym
bull nozologia DH jest zwodnicza dla wspoacutełczesnej społeczności
zwłaszcza niedermatologicznej
(opryszczkopodobne zapalenie skoacutery)
bull kontinuum autoimmunizacji i (auto)zapalenia
bull kluczowymi w skoacuternej patologii jawią się eTG i neutrofil
(uchwycenie zjawisk skoacuternych jak najbardziej DH-specyficznych)
bull DH to zapewne choroba skoacuterna z towarzyszącą nadwrażliwością na gluten
nieporozumienia
bull dapson na import docelowy
bull okolica łokciowa
bull pośladek jako miejsce wykonania DIFf
bull
foto Zbyszek KaczmarekGazeta Polska
Mężczyzna lat 77
Oral Surg Oral Med Oral Pathol 1982 Jul54(1)22-5
Dermatitis herpetiformis IgA deposits in gingiva buccal
mucosa and skin
Nisengard RJ Chorzelski T Maciejowska E Kryst L
Abstract
Fourteen patients who had dermatitis herpetiformis of the skin with no
gingival lesions were studied In each patient biopsy specimens of
normal gingiva buccal mucosa and perilesional skin were examined
for IgA and IgG deposits Depending on the method of handling
biopsy specimens for immunofluorescence IgA deposits were
detected in 21 to 25 percent of gingival specimens 27 to 46 percent
of buccal mucosal specimens and 64 to 76 percent of skin
specimens The occurrence of IgA deposits in the gingival papillae a
site where lesions of DH have not been reported in the past or
observed in this study suggests that these IgA deposits alone may
not play a primary role in the pathogenesis of this disease Similar
immunofluorescent findings of IgA deposits were observed in both
quick-frozen biopsy specimens and those placed in holding solution
indicating the suitability of the holding solution for transporting
suggested DH biopsy material
PMID 6750497 [PubMed - indexed for MEDLINE]
We hypothesize that the IgA class
anti-TG3 Abs are directly
responsible
for the immune deposits and that
the TG3 is from human epidermis
as this is its only source in our
model
Epidermal transglutaminase
Patients with DH had elevated levels of IgA anti-TG3 (Fig 2) Twenty-three of 44 (52) had IgA anti-TG3 levels
gt 18 units
Wyniki Zaledwie u 8 spośroacuted 21
(38) chorych na DH stwierdzono że
wyniki badań TG3 IF oraz badań IgA
TG3 ELISA były zbieżne (wyniki badań
obiema
metodami pozytywne oraz wyniki
badań obiema metodami negatywne)
Wnioski Wyniki niniejszego
doniesienia zdają się sugerować że u
chorych na DH zjawiska zależne od
TG3 na poziomie krwiobiegu i na
poziomie skoacuternym
nie są jeżeli chodzi o patogenezę tej
choroby powiązane w znaczącym
stopniu
Cutaneous expression of neutrophil elastase in relation
to IgA antibodies to nonapeptides of gliadin and
tissue transglutaminase in dermatitis
herpetiformis
Results
NE (top left) deposits in immunohistochemistry in
lesional skin in a male patient with DH
(immunoperoxidase staining on paraffin embedded
sections original magnification x200)
Intensity of NE (bottom left) deposits processed
with digital microscopic image analysis
superimposed on NE deposits
in immunohistochemistry in lesional skin in
this patient
Intensity of NE (top right) deposits processed with
digital microscopic image analysis in lesional skin in
this patient
Conclusions
bull Thus it seems that the production of IgA npG takes place in a coordinated way with the production of IgA tTG when patients show cutaneous lesions of DH
bull Nevertheless it is hypothesized that IgA npG and IgA tTG regardless of the issue of their diagnostic significance have lesser importance as far as cutaneous pathology of human DH mediated by DEJ-degrading NE released from IgA autoimmunity-activated neutrophils is concerned
Consistently with the autoimmune
origin of DH functional classification
of the differentially expressed genes
(DEGs) indicates a B- and T-cell
immune response (LAG3 TRAF5
DPP4 and NT5E) In addition gene
modulation provides evidence for a
local inflammatory response (IL8
PTGFR FSTL1 IFI16 BDKRD2
and NAMPT) with concomitant
leukocyte recruitment (CCL5
ENPP2) endothelial cell activation
and neutrophil extravasation (SELL
SELE) DEGs also indicate
overproduction of matrix proteases
(MMP9 ADAM9 and ADAM19) and
proteolytic enzymes (CTSG ELA2
CPA3 TPSB2 and CMA1) that may
contribute to epidermal splitting and
blister formation
In conclusion our data add DH
plaque psoriasis and
psoriatic arthritis to the growing
list of disorders associated
with Ig deregulation where the
enhancer HS12-A may be
involved
The incubation with Ni-Ti heat-
activated (T3) or Ni-Ti super-elastic
(T4) and with Ni-Cr-Co (T2) alloys
produced respectively 25-fold and 8-
fold increases in IL-6 release
compared with control cultures
Transglutaminase activity was
significantly increased in cells
exposed to T3 and T4 alloys (about
170 of control p lt 005) where it
was mainly localized close to inner
part of cell membrane The exposure
to T3 and T4 specimens significantly
up-regulated also tTG expression
compared with control cultures
These data first show an association
between IL-6 release and tissue
transglutaminase increases
suggesting that TGase-mediated
reactions may play a major role in
periodontal inflammation
pp 178-9
DH patomechanizm
Uważam że należy postrzegać DH jako chorobę skoacuterną z drugorzędnym udziałem patologii jelitowej
Sądzę że w skoacuternej patogenezie tej dermatozy wspoacutełgrają wzajemnie zapętlone zjawiska autoimmunizacji zależne od kluczowego autoantygenu ndash enzymu transglutaminazy naskoacuterkowej (eTG) przemieszczonej być może w wyniku mikrourazoacutew i drapania do skoacutery właściwej w bliskości połączenia skoacuterno-naskoacuterkowego (dermal-epidermal junction DEJ) z wyższych warstw naskoacuterka gdzie ma ona znaczenie fizjologiczne jako bdquoklej biologicznyrdquo (jeden z elementoacutew bdquobariery naskoacuterkowejrdquobdquokoperty rogowejrdquo) oraz (auto)zapalenia zależnego od uczynnionych neutrofiloacutew uwalniających elastazę neutrofiloacutew (NE) trawiącą DEJ z wytworzeniem rozwarstwienia w przestrzeni lamina lucida
DH postępowanie diagnostyczne
Standardem diagnostyki roacuteżnicowej DH powinno być postępowanie troacutejskładnikowe oparte o badanie kliniczne (co i gdzie)(stereotypowym chorym będzie młodzieniec lub młody mężczyzna) bezpośrednie badanie immunofluorescencyjne (DIF)skoacutery klinicznie niezmienionej z otoczenia wykwitoacutew analogicznie do pozostałych autoimmunizacyjnych dermatoz pęcherzowych (ujawnia definiujące to schorzenie złogi IgA w co najmniej 7 wzorach) oraz oznaczenie surowiczych przeciwciał IgA techniką ELISA z jednym substratem do wyboru z zakresu transglutaminaza tkankowa (tTG) eTG nonapeptydy gliadyny (npG) neoepitopy gliadyna-tTG (neo-tTG) Owo postępowanie można uzupełnić o badanie histologiczne H+E wycinka ze skoacutery wykwitowej i badanie haplotypu HLA DQ2DQ8 u chorych z niejednoznacznym obrazem kliniczno-pracownianym
DH postępowanie lecznicze
Standardem terapeutycznym w DH czyli generalnie postępowaniem terapeutycznym z wyboru powinno natomiast być postępowanie dwuskładnikowe czyli powiązanie leczenia farmakologicznego kluczowym dapsonem i dietetycznego dietą bezglutenową w indywidualizowanych kombinacjach W postępowaniu leczniczym trzeba też uwzględnić całość problemoacutew zdrowotnych chorego
ACTA DERMATO-VENEREOLOGICA REVIEWERacuteS COMMENTS TO THE AUTHOR(S) Re Manuscript 114366 Authors Pasternack et al Title Quality of life and gastrointestinal symptoms in long-term g The authors analysed the HRQoL in DH patients on gluten free diet The topic is interesting however the study design is questionable First af all dermatitis herpetiformis is not a cutaneous manifestation of coeliac disease but it is rather a cutaneous disease associated with coeliac disease Furthermore the healthy group is poorly characterized (eg concomitant diseases are not mentioned at all eg Diabetes arterial hypertension) No comparison was performed regarding the age and gender distribution between DH patients and controls As there are differences within the DH patients regarding males and females a very low proportion of men in control group is an important bias as it seems that gender may be relevant cofactor In addition I would rather expect comparison between DH menhealthy men and DH womenhealthy women rather than between DH menDH women as the HRQOL in DH patients has been shown to be similar to controls The authors claimed that having ongoing skin symptoms at the time of the study had no influence on GSRS PGWB or SF-36 scores and the data are not shown In my opinion it is very probable that lack of significance was related to very small number of patients in the group of active skin lesions I would also expect from the authors to provide the information about concomitant gastrointestinal symptoms at the time of DH diagnosis It is probable that many of these patients never had clinically relevant symptoms of coeliac disease and thus GSRS would rather assess the effect of gluten-free diet on gastrointestinal symptoms instead of the relevance of coeliac disease symptomatology
Opryszczkowate zapalenie skoacutery jest
schorzeniem skoacuternym
bull nozologia DH jest zwodnicza dla wspoacutełczesnej społeczności
zwłaszcza niedermatologicznej
(opryszczkopodobne zapalenie skoacutery)
bull kontinuum autoimmunizacji i (auto)zapalenia
bull kluczowymi w skoacuternej patologii jawią się eTG i neutrofil
(uchwycenie zjawisk skoacuternych jak najbardziej DH-specyficznych)
bull DH to zapewne choroba skoacuterna z towarzyszącą nadwrażliwością na gluten
nieporozumienia
bull dapson na import docelowy
bull okolica łokciowa
bull pośladek jako miejsce wykonania DIFf
bull
foto Zbyszek KaczmarekGazeta Polska

Oral Surg Oral Med Oral Pathol 1982 Jul54(1)22-5
Dermatitis herpetiformis IgA deposits in gingiva buccal
mucosa and skin
Nisengard RJ Chorzelski T Maciejowska E Kryst L
Abstract
Fourteen patients who had dermatitis herpetiformis of the skin with no
gingival lesions were studied In each patient biopsy specimens of
normal gingiva buccal mucosa and perilesional skin were examined
for IgA and IgG deposits Depending on the method of handling
biopsy specimens for immunofluorescence IgA deposits were
detected in 21 to 25 percent of gingival specimens 27 to 46 percent
of buccal mucosal specimens and 64 to 76 percent of skin
specimens The occurrence of IgA deposits in the gingival papillae a
site where lesions of DH have not been reported in the past or
observed in this study suggests that these IgA deposits alone may
not play a primary role in the pathogenesis of this disease Similar
immunofluorescent findings of IgA deposits were observed in both
quick-frozen biopsy specimens and those placed in holding solution
indicating the suitability of the holding solution for transporting
suggested DH biopsy material
PMID 6750497 [PubMed - indexed for MEDLINE]
We hypothesize that the IgA class
anti-TG3 Abs are directly
responsible
for the immune deposits and that
the TG3 is from human epidermis
as this is its only source in our
model
Epidermal transglutaminase
Patients with DH had elevated levels of IgA anti-TG3 (Fig 2) Twenty-three of 44 (52) had IgA anti-TG3 levels
gt 18 units
Wyniki Zaledwie u 8 spośroacuted 21
(38) chorych na DH stwierdzono że
wyniki badań TG3 IF oraz badań IgA
TG3 ELISA były zbieżne (wyniki badań
obiema
metodami pozytywne oraz wyniki
badań obiema metodami negatywne)
Wnioski Wyniki niniejszego
doniesienia zdają się sugerować że u
chorych na DH zjawiska zależne od
TG3 na poziomie krwiobiegu i na
poziomie skoacuternym
nie są jeżeli chodzi o patogenezę tej
choroby powiązane w znaczącym
stopniu
Cutaneous expression of neutrophil elastase in relation
to IgA antibodies to nonapeptides of gliadin and
tissue transglutaminase in dermatitis
herpetiformis
Results
NE (top left) deposits in immunohistochemistry in
lesional skin in a male patient with DH
(immunoperoxidase staining on paraffin embedded
sections original magnification x200)
Intensity of NE (bottom left) deposits processed
with digital microscopic image analysis
superimposed on NE deposits
in immunohistochemistry in lesional skin in
this patient
Intensity of NE (top right) deposits processed with
digital microscopic image analysis in lesional skin in
this patient
Conclusions
bull Thus it seems that the production of IgA npG takes place in a coordinated way with the production of IgA tTG when patients show cutaneous lesions of DH
bull Nevertheless it is hypothesized that IgA npG and IgA tTG regardless of the issue of their diagnostic significance have lesser importance as far as cutaneous pathology of human DH mediated by DEJ-degrading NE released from IgA autoimmunity-activated neutrophils is concerned
Consistently with the autoimmune
origin of DH functional classification
of the differentially expressed genes
(DEGs) indicates a B- and T-cell
immune response (LAG3 TRAF5
DPP4 and NT5E) In addition gene
modulation provides evidence for a
local inflammatory response (IL8
PTGFR FSTL1 IFI16 BDKRD2
and NAMPT) with concomitant
leukocyte recruitment (CCL5
ENPP2) endothelial cell activation
and neutrophil extravasation (SELL
SELE) DEGs also indicate
overproduction of matrix proteases
(MMP9 ADAM9 and ADAM19) and
proteolytic enzymes (CTSG ELA2
CPA3 TPSB2 and CMA1) that may
contribute to epidermal splitting and
blister formation
In conclusion our data add DH
plaque psoriasis and
psoriatic arthritis to the growing
list of disorders associated
with Ig deregulation where the
enhancer HS12-A may be
involved
The incubation with Ni-Ti heat-
activated (T3) or Ni-Ti super-elastic
(T4) and with Ni-Cr-Co (T2) alloys
produced respectively 25-fold and 8-
fold increases in IL-6 release
compared with control cultures
Transglutaminase activity was
significantly increased in cells
exposed to T3 and T4 alloys (about
170 of control p lt 005) where it
was mainly localized close to inner
part of cell membrane The exposure
to T3 and T4 specimens significantly
up-regulated also tTG expression
compared with control cultures
These data first show an association
between IL-6 release and tissue
transglutaminase increases
suggesting that TGase-mediated
reactions may play a major role in
periodontal inflammation
pp 178-9
DH patomechanizm
Uważam że należy postrzegać DH jako chorobę skoacuterną z drugorzędnym udziałem patologii jelitowej
Sądzę że w skoacuternej patogenezie tej dermatozy wspoacutełgrają wzajemnie zapętlone zjawiska autoimmunizacji zależne od kluczowego autoantygenu ndash enzymu transglutaminazy naskoacuterkowej (eTG) przemieszczonej być może w wyniku mikrourazoacutew i drapania do skoacutery właściwej w bliskości połączenia skoacuterno-naskoacuterkowego (dermal-epidermal junction DEJ) z wyższych warstw naskoacuterka gdzie ma ona znaczenie fizjologiczne jako bdquoklej biologicznyrdquo (jeden z elementoacutew bdquobariery naskoacuterkowejrdquobdquokoperty rogowejrdquo) oraz (auto)zapalenia zależnego od uczynnionych neutrofiloacutew uwalniających elastazę neutrofiloacutew (NE) trawiącą DEJ z wytworzeniem rozwarstwienia w przestrzeni lamina lucida
DH postępowanie diagnostyczne
Standardem diagnostyki roacuteżnicowej DH powinno być postępowanie troacutejskładnikowe oparte o badanie kliniczne (co i gdzie)(stereotypowym chorym będzie młodzieniec lub młody mężczyzna) bezpośrednie badanie immunofluorescencyjne (DIF)skoacutery klinicznie niezmienionej z otoczenia wykwitoacutew analogicznie do pozostałych autoimmunizacyjnych dermatoz pęcherzowych (ujawnia definiujące to schorzenie złogi IgA w co najmniej 7 wzorach) oraz oznaczenie surowiczych przeciwciał IgA techniką ELISA z jednym substratem do wyboru z zakresu transglutaminaza tkankowa (tTG) eTG nonapeptydy gliadyny (npG) neoepitopy gliadyna-tTG (neo-tTG) Owo postępowanie można uzupełnić o badanie histologiczne H+E wycinka ze skoacutery wykwitowej i badanie haplotypu HLA DQ2DQ8 u chorych z niejednoznacznym obrazem kliniczno-pracownianym
DH postępowanie lecznicze
Standardem terapeutycznym w DH czyli generalnie postępowaniem terapeutycznym z wyboru powinno natomiast być postępowanie dwuskładnikowe czyli powiązanie leczenia farmakologicznego kluczowym dapsonem i dietetycznego dietą bezglutenową w indywidualizowanych kombinacjach W postępowaniu leczniczym trzeba też uwzględnić całość problemoacutew zdrowotnych chorego
ACTA DERMATO-VENEREOLOGICA REVIEWERacuteS COMMENTS TO THE AUTHOR(S) Re Manuscript 114366 Authors Pasternack et al Title Quality of life and gastrointestinal symptoms in long-term g The authors analysed the HRQoL in DH patients on gluten free diet The topic is interesting however the study design is questionable First af all dermatitis herpetiformis is not a cutaneous manifestation of coeliac disease but it is rather a cutaneous disease associated with coeliac disease Furthermore the healthy group is poorly characterized (eg concomitant diseases are not mentioned at all eg Diabetes arterial hypertension) No comparison was performed regarding the age and gender distribution between DH patients and controls As there are differences within the DH patients regarding males and females a very low proportion of men in control group is an important bias as it seems that gender may be relevant cofactor In addition I would rather expect comparison between DH menhealthy men and DH womenhealthy women rather than between DH menDH women as the HRQOL in DH patients has been shown to be similar to controls The authors claimed that having ongoing skin symptoms at the time of the study had no influence on GSRS PGWB or SF-36 scores and the data are not shown In my opinion it is very probable that lack of significance was related to very small number of patients in the group of active skin lesions I would also expect from the authors to provide the information about concomitant gastrointestinal symptoms at the time of DH diagnosis It is probable that many of these patients never had clinically relevant symptoms of coeliac disease and thus GSRS would rather assess the effect of gluten-free diet on gastrointestinal symptoms instead of the relevance of coeliac disease symptomatology
Opryszczkowate zapalenie skoacutery jest
schorzeniem skoacuternym
bull nozologia DH jest zwodnicza dla wspoacutełczesnej społeczności
zwłaszcza niedermatologicznej
(opryszczkopodobne zapalenie skoacutery)
bull kontinuum autoimmunizacji i (auto)zapalenia
bull kluczowymi w skoacuternej patologii jawią się eTG i neutrofil
(uchwycenie zjawisk skoacuternych jak najbardziej DH-specyficznych)
bull DH to zapewne choroba skoacuterna z towarzyszącą nadwrażliwością na gluten
nieporozumienia
bull dapson na import docelowy
bull okolica łokciowa
bull pośladek jako miejsce wykonania DIFf
bull
foto Zbyszek KaczmarekGazeta Polska

We hypothesize that the IgA class
anti-TG3 Abs are directly
responsible
for the immune deposits and that
the TG3 is from human epidermis
as this is its only source in our
model
Epidermal transglutaminase
Patients with DH had elevated levels of IgA anti-TG3 (Fig 2) Twenty-three of 44 (52) had IgA anti-TG3 levels
gt 18 units
Wyniki Zaledwie u 8 spośroacuted 21
(38) chorych na DH stwierdzono że
wyniki badań TG3 IF oraz badań IgA
TG3 ELISA były zbieżne (wyniki badań
obiema
metodami pozytywne oraz wyniki
badań obiema metodami negatywne)
Wnioski Wyniki niniejszego
doniesienia zdają się sugerować że u
chorych na DH zjawiska zależne od
TG3 na poziomie krwiobiegu i na
poziomie skoacuternym
nie są jeżeli chodzi o patogenezę tej
choroby powiązane w znaczącym
stopniu
Cutaneous expression of neutrophil elastase in relation
to IgA antibodies to nonapeptides of gliadin and
tissue transglutaminase in dermatitis
herpetiformis
Results
NE (top left) deposits in immunohistochemistry in
lesional skin in a male patient with DH
(immunoperoxidase staining on paraffin embedded
sections original magnification x200)
Intensity of NE (bottom left) deposits processed
with digital microscopic image analysis
superimposed on NE deposits
in immunohistochemistry in lesional skin in
this patient
Intensity of NE (top right) deposits processed with
digital microscopic image analysis in lesional skin in
this patient
Conclusions
bull Thus it seems that the production of IgA npG takes place in a coordinated way with the production of IgA tTG when patients show cutaneous lesions of DH
bull Nevertheless it is hypothesized that IgA npG and IgA tTG regardless of the issue of their diagnostic significance have lesser importance as far as cutaneous pathology of human DH mediated by DEJ-degrading NE released from IgA autoimmunity-activated neutrophils is concerned
Consistently with the autoimmune
origin of DH functional classification
of the differentially expressed genes
(DEGs) indicates a B- and T-cell
immune response (LAG3 TRAF5
DPP4 and NT5E) In addition gene
modulation provides evidence for a
local inflammatory response (IL8
PTGFR FSTL1 IFI16 BDKRD2
and NAMPT) with concomitant
leukocyte recruitment (CCL5
ENPP2) endothelial cell activation
and neutrophil extravasation (SELL
SELE) DEGs also indicate
overproduction of matrix proteases
(MMP9 ADAM9 and ADAM19) and
proteolytic enzymes (CTSG ELA2
CPA3 TPSB2 and CMA1) that may
contribute to epidermal splitting and
blister formation
In conclusion our data add DH
plaque psoriasis and
psoriatic arthritis to the growing
list of disorders associated
with Ig deregulation where the
enhancer HS12-A may be
involved
The incubation with Ni-Ti heat-
activated (T3) or Ni-Ti super-elastic
(T4) and with Ni-Cr-Co (T2) alloys
produced respectively 25-fold and 8-
fold increases in IL-6 release
compared with control cultures
Transglutaminase activity was
significantly increased in cells
exposed to T3 and T4 alloys (about
170 of control p lt 005) where it
was mainly localized close to inner
part of cell membrane The exposure
to T3 and T4 specimens significantly
up-regulated also tTG expression
compared with control cultures
These data first show an association
between IL-6 release and tissue
transglutaminase increases
suggesting that TGase-mediated
reactions may play a major role in
periodontal inflammation
pp 178-9
DH patomechanizm
Uważam że należy postrzegać DH jako chorobę skoacuterną z drugorzędnym udziałem patologii jelitowej
Sądzę że w skoacuternej patogenezie tej dermatozy wspoacutełgrają wzajemnie zapętlone zjawiska autoimmunizacji zależne od kluczowego autoantygenu ndash enzymu transglutaminazy naskoacuterkowej (eTG) przemieszczonej być może w wyniku mikrourazoacutew i drapania do skoacutery właściwej w bliskości połączenia skoacuterno-naskoacuterkowego (dermal-epidermal junction DEJ) z wyższych warstw naskoacuterka gdzie ma ona znaczenie fizjologiczne jako bdquoklej biologicznyrdquo (jeden z elementoacutew bdquobariery naskoacuterkowejrdquobdquokoperty rogowejrdquo) oraz (auto)zapalenia zależnego od uczynnionych neutrofiloacutew uwalniających elastazę neutrofiloacutew (NE) trawiącą DEJ z wytworzeniem rozwarstwienia w przestrzeni lamina lucida
DH postępowanie diagnostyczne
Standardem diagnostyki roacuteżnicowej DH powinno być postępowanie troacutejskładnikowe oparte o badanie kliniczne (co i gdzie)(stereotypowym chorym będzie młodzieniec lub młody mężczyzna) bezpośrednie badanie immunofluorescencyjne (DIF)skoacutery klinicznie niezmienionej z otoczenia wykwitoacutew analogicznie do pozostałych autoimmunizacyjnych dermatoz pęcherzowych (ujawnia definiujące to schorzenie złogi IgA w co najmniej 7 wzorach) oraz oznaczenie surowiczych przeciwciał IgA techniką ELISA z jednym substratem do wyboru z zakresu transglutaminaza tkankowa (tTG) eTG nonapeptydy gliadyny (npG) neoepitopy gliadyna-tTG (neo-tTG) Owo postępowanie można uzupełnić o badanie histologiczne H+E wycinka ze skoacutery wykwitowej i badanie haplotypu HLA DQ2DQ8 u chorych z niejednoznacznym obrazem kliniczno-pracownianym
DH postępowanie lecznicze
Standardem terapeutycznym w DH czyli generalnie postępowaniem terapeutycznym z wyboru powinno natomiast być postępowanie dwuskładnikowe czyli powiązanie leczenia farmakologicznego kluczowym dapsonem i dietetycznego dietą bezglutenową w indywidualizowanych kombinacjach W postępowaniu leczniczym trzeba też uwzględnić całość problemoacutew zdrowotnych chorego
ACTA DERMATO-VENEREOLOGICA REVIEWERacuteS COMMENTS TO THE AUTHOR(S) Re Manuscript 114366 Authors Pasternack et al Title Quality of life and gastrointestinal symptoms in long-term g The authors analysed the HRQoL in DH patients on gluten free diet The topic is interesting however the study design is questionable First af all dermatitis herpetiformis is not a cutaneous manifestation of coeliac disease but it is rather a cutaneous disease associated with coeliac disease Furthermore the healthy group is poorly characterized (eg concomitant diseases are not mentioned at all eg Diabetes arterial hypertension) No comparison was performed regarding the age and gender distribution between DH patients and controls As there are differences within the DH patients regarding males and females a very low proportion of men in control group is an important bias as it seems that gender may be relevant cofactor In addition I would rather expect comparison between DH menhealthy men and DH womenhealthy women rather than between DH menDH women as the HRQOL in DH patients has been shown to be similar to controls The authors claimed that having ongoing skin symptoms at the time of the study had no influence on GSRS PGWB or SF-36 scores and the data are not shown In my opinion it is very probable that lack of significance was related to very small number of patients in the group of active skin lesions I would also expect from the authors to provide the information about concomitant gastrointestinal symptoms at the time of DH diagnosis It is probable that many of these patients never had clinically relevant symptoms of coeliac disease and thus GSRS would rather assess the effect of gluten-free diet on gastrointestinal symptoms instead of the relevance of coeliac disease symptomatology
Opryszczkowate zapalenie skoacutery jest
schorzeniem skoacuternym
bull nozologia DH jest zwodnicza dla wspoacutełczesnej społeczności
zwłaszcza niedermatologicznej
(opryszczkopodobne zapalenie skoacutery)
bull kontinuum autoimmunizacji i (auto)zapalenia
bull kluczowymi w skoacuternej patologii jawią się eTG i neutrofil
(uchwycenie zjawisk skoacuternych jak najbardziej DH-specyficznych)
bull DH to zapewne choroba skoacuterna z towarzyszącą nadwrażliwością na gluten
nieporozumienia
bull dapson na import docelowy
bull okolica łokciowa
bull pośladek jako miejsce wykonania DIFf
bull
foto Zbyszek KaczmarekGazeta Polska
Epidermal transglutaminase
Patients with DH had elevated levels of IgA anti-TG3 (Fig 2) Twenty-three of 44 (52) had IgA anti-TG3 levels
gt 18 units
Wyniki Zaledwie u 8 spośroacuted 21
(38) chorych na DH stwierdzono że
wyniki badań TG3 IF oraz badań IgA
TG3 ELISA były zbieżne (wyniki badań
obiema
metodami pozytywne oraz wyniki
badań obiema metodami negatywne)
Wnioski Wyniki niniejszego
doniesienia zdają się sugerować że u
chorych na DH zjawiska zależne od
TG3 na poziomie krwiobiegu i na
poziomie skoacuternym
nie są jeżeli chodzi o patogenezę tej
choroby powiązane w znaczącym
stopniu
Cutaneous expression of neutrophil elastase in relation
to IgA antibodies to nonapeptides of gliadin and
tissue transglutaminase in dermatitis
herpetiformis
Results
NE (top left) deposits in immunohistochemistry in
lesional skin in a male patient with DH
(immunoperoxidase staining on paraffin embedded
sections original magnification x200)
Intensity of NE (bottom left) deposits processed
with digital microscopic image analysis
superimposed on NE deposits
in immunohistochemistry in lesional skin in
this patient
Intensity of NE (top right) deposits processed with
digital microscopic image analysis in lesional skin in
this patient
Conclusions
bull Thus it seems that the production of IgA npG takes place in a coordinated way with the production of IgA tTG when patients show cutaneous lesions of DH
bull Nevertheless it is hypothesized that IgA npG and IgA tTG regardless of the issue of their diagnostic significance have lesser importance as far as cutaneous pathology of human DH mediated by DEJ-degrading NE released from IgA autoimmunity-activated neutrophils is concerned
Consistently with the autoimmune
origin of DH functional classification
of the differentially expressed genes
(DEGs) indicates a B- and T-cell
immune response (LAG3 TRAF5
DPP4 and NT5E) In addition gene
modulation provides evidence for a
local inflammatory response (IL8
PTGFR FSTL1 IFI16 BDKRD2
and NAMPT) with concomitant
leukocyte recruitment (CCL5
ENPP2) endothelial cell activation
and neutrophil extravasation (SELL
SELE) DEGs also indicate
overproduction of matrix proteases
(MMP9 ADAM9 and ADAM19) and
proteolytic enzymes (CTSG ELA2
CPA3 TPSB2 and CMA1) that may
contribute to epidermal splitting and
blister formation
In conclusion our data add DH
plaque psoriasis and
psoriatic arthritis to the growing
list of disorders associated
with Ig deregulation where the
enhancer HS12-A may be
involved
The incubation with Ni-Ti heat-
activated (T3) or Ni-Ti super-elastic
(T4) and with Ni-Cr-Co (T2) alloys
produced respectively 25-fold and 8-
fold increases in IL-6 release
compared with control cultures
Transglutaminase activity was
significantly increased in cells
exposed to T3 and T4 alloys (about
170 of control p lt 005) where it
was mainly localized close to inner
part of cell membrane The exposure
to T3 and T4 specimens significantly
up-regulated also tTG expression
compared with control cultures
These data first show an association
between IL-6 release and tissue
transglutaminase increases
suggesting that TGase-mediated
reactions may play a major role in
periodontal inflammation
pp 178-9
DH patomechanizm
Uważam że należy postrzegać DH jako chorobę skoacuterną z drugorzędnym udziałem patologii jelitowej
Sądzę że w skoacuternej patogenezie tej dermatozy wspoacutełgrają wzajemnie zapętlone zjawiska autoimmunizacji zależne od kluczowego autoantygenu ndash enzymu transglutaminazy naskoacuterkowej (eTG) przemieszczonej być może w wyniku mikrourazoacutew i drapania do skoacutery właściwej w bliskości połączenia skoacuterno-naskoacuterkowego (dermal-epidermal junction DEJ) z wyższych warstw naskoacuterka gdzie ma ona znaczenie fizjologiczne jako bdquoklej biologicznyrdquo (jeden z elementoacutew bdquobariery naskoacuterkowejrdquobdquokoperty rogowejrdquo) oraz (auto)zapalenia zależnego od uczynnionych neutrofiloacutew uwalniających elastazę neutrofiloacutew (NE) trawiącą DEJ z wytworzeniem rozwarstwienia w przestrzeni lamina lucida
DH postępowanie diagnostyczne
Standardem diagnostyki roacuteżnicowej DH powinno być postępowanie troacutejskładnikowe oparte o badanie kliniczne (co i gdzie)(stereotypowym chorym będzie młodzieniec lub młody mężczyzna) bezpośrednie badanie immunofluorescencyjne (DIF)skoacutery klinicznie niezmienionej z otoczenia wykwitoacutew analogicznie do pozostałych autoimmunizacyjnych dermatoz pęcherzowych (ujawnia definiujące to schorzenie złogi IgA w co najmniej 7 wzorach) oraz oznaczenie surowiczych przeciwciał IgA techniką ELISA z jednym substratem do wyboru z zakresu transglutaminaza tkankowa (tTG) eTG nonapeptydy gliadyny (npG) neoepitopy gliadyna-tTG (neo-tTG) Owo postępowanie można uzupełnić o badanie histologiczne H+E wycinka ze skoacutery wykwitowej i badanie haplotypu HLA DQ2DQ8 u chorych z niejednoznacznym obrazem kliniczno-pracownianym
DH postępowanie lecznicze
Standardem terapeutycznym w DH czyli generalnie postępowaniem terapeutycznym z wyboru powinno natomiast być postępowanie dwuskładnikowe czyli powiązanie leczenia farmakologicznego kluczowym dapsonem i dietetycznego dietą bezglutenową w indywidualizowanych kombinacjach W postępowaniu leczniczym trzeba też uwzględnić całość problemoacutew zdrowotnych chorego
ACTA DERMATO-VENEREOLOGICA REVIEWERacuteS COMMENTS TO THE AUTHOR(S) Re Manuscript 114366 Authors Pasternack et al Title Quality of life and gastrointestinal symptoms in long-term g The authors analysed the HRQoL in DH patients on gluten free diet The topic is interesting however the study design is questionable First af all dermatitis herpetiformis is not a cutaneous manifestation of coeliac disease but it is rather a cutaneous disease associated with coeliac disease Furthermore the healthy group is poorly characterized (eg concomitant diseases are not mentioned at all eg Diabetes arterial hypertension) No comparison was performed regarding the age and gender distribution between DH patients and controls As there are differences within the DH patients regarding males and females a very low proportion of men in control group is an important bias as it seems that gender may be relevant cofactor In addition I would rather expect comparison between DH menhealthy men and DH womenhealthy women rather than between DH menDH women as the HRQOL in DH patients has been shown to be similar to controls The authors claimed that having ongoing skin symptoms at the time of the study had no influence on GSRS PGWB or SF-36 scores and the data are not shown In my opinion it is very probable that lack of significance was related to very small number of patients in the group of active skin lesions I would also expect from the authors to provide the information about concomitant gastrointestinal symptoms at the time of DH diagnosis It is probable that many of these patients never had clinically relevant symptoms of coeliac disease and thus GSRS would rather assess the effect of gluten-free diet on gastrointestinal symptoms instead of the relevance of coeliac disease symptomatology
Opryszczkowate zapalenie skoacutery jest
schorzeniem skoacuternym
bull nozologia DH jest zwodnicza dla wspoacutełczesnej społeczności
zwłaszcza niedermatologicznej
(opryszczkopodobne zapalenie skoacutery)
bull kontinuum autoimmunizacji i (auto)zapalenia
bull kluczowymi w skoacuternej patologii jawią się eTG i neutrofil
(uchwycenie zjawisk skoacuternych jak najbardziej DH-specyficznych)
bull DH to zapewne choroba skoacuterna z towarzyszącą nadwrażliwością na gluten
nieporozumienia
bull dapson na import docelowy
bull okolica łokciowa
bull pośladek jako miejsce wykonania DIFf
bull
foto Zbyszek KaczmarekGazeta Polska
Wyniki Zaledwie u 8 spośroacuted 21
(38) chorych na DH stwierdzono że
wyniki badań TG3 IF oraz badań IgA
TG3 ELISA były zbieżne (wyniki badań
obiema
metodami pozytywne oraz wyniki
badań obiema metodami negatywne)
Wnioski Wyniki niniejszego
doniesienia zdają się sugerować że u
chorych na DH zjawiska zależne od
TG3 na poziomie krwiobiegu i na
poziomie skoacuternym
nie są jeżeli chodzi o patogenezę tej
choroby powiązane w znaczącym
stopniu
Cutaneous expression of neutrophil elastase in relation
to IgA antibodies to nonapeptides of gliadin and
tissue transglutaminase in dermatitis
herpetiformis
Results
NE (top left) deposits in immunohistochemistry in
lesional skin in a male patient with DH
(immunoperoxidase staining on paraffin embedded
sections original magnification x200)
Intensity of NE (bottom left) deposits processed
with digital microscopic image analysis
superimposed on NE deposits
in immunohistochemistry in lesional skin in
this patient
Intensity of NE (top right) deposits processed with
digital microscopic image analysis in lesional skin in
this patient
Conclusions
bull Thus it seems that the production of IgA npG takes place in a coordinated way with the production of IgA tTG when patients show cutaneous lesions of DH
bull Nevertheless it is hypothesized that IgA npG and IgA tTG regardless of the issue of their diagnostic significance have lesser importance as far as cutaneous pathology of human DH mediated by DEJ-degrading NE released from IgA autoimmunity-activated neutrophils is concerned
Consistently with the autoimmune
origin of DH functional classification
of the differentially expressed genes
(DEGs) indicates a B- and T-cell
immune response (LAG3 TRAF5
DPP4 and NT5E) In addition gene
modulation provides evidence for a
local inflammatory response (IL8
PTGFR FSTL1 IFI16 BDKRD2
and NAMPT) with concomitant
leukocyte recruitment (CCL5
ENPP2) endothelial cell activation
and neutrophil extravasation (SELL
SELE) DEGs also indicate
overproduction of matrix proteases
(MMP9 ADAM9 and ADAM19) and
proteolytic enzymes (CTSG ELA2
CPA3 TPSB2 and CMA1) that may
contribute to epidermal splitting and
blister formation
In conclusion our data add DH
plaque psoriasis and
psoriatic arthritis to the growing
list of disorders associated
with Ig deregulation where the
enhancer HS12-A may be
involved
The incubation with Ni-Ti heat-
activated (T3) or Ni-Ti super-elastic
(T4) and with Ni-Cr-Co (T2) alloys
produced respectively 25-fold and 8-
fold increases in IL-6 release
compared with control cultures
Transglutaminase activity was
significantly increased in cells
exposed to T3 and T4 alloys (about
170 of control p lt 005) where it
was mainly localized close to inner
part of cell membrane The exposure
to T3 and T4 specimens significantly
up-regulated also tTG expression
compared with control cultures
These data first show an association
between IL-6 release and tissue
transglutaminase increases
suggesting that TGase-mediated
reactions may play a major role in
periodontal inflammation
pp 178-9
DH patomechanizm
Uważam że należy postrzegać DH jako chorobę skoacuterną z drugorzędnym udziałem patologii jelitowej
Sądzę że w skoacuternej patogenezie tej dermatozy wspoacutełgrają wzajemnie zapętlone zjawiska autoimmunizacji zależne od kluczowego autoantygenu ndash enzymu transglutaminazy naskoacuterkowej (eTG) przemieszczonej być może w wyniku mikrourazoacutew i drapania do skoacutery właściwej w bliskości połączenia skoacuterno-naskoacuterkowego (dermal-epidermal junction DEJ) z wyższych warstw naskoacuterka gdzie ma ona znaczenie fizjologiczne jako bdquoklej biologicznyrdquo (jeden z elementoacutew bdquobariery naskoacuterkowejrdquobdquokoperty rogowejrdquo) oraz (auto)zapalenia zależnego od uczynnionych neutrofiloacutew uwalniających elastazę neutrofiloacutew (NE) trawiącą DEJ z wytworzeniem rozwarstwienia w przestrzeni lamina lucida
DH postępowanie diagnostyczne
Standardem diagnostyki roacuteżnicowej DH powinno być postępowanie troacutejskładnikowe oparte o badanie kliniczne (co i gdzie)(stereotypowym chorym będzie młodzieniec lub młody mężczyzna) bezpośrednie badanie immunofluorescencyjne (DIF)skoacutery klinicznie niezmienionej z otoczenia wykwitoacutew analogicznie do pozostałych autoimmunizacyjnych dermatoz pęcherzowych (ujawnia definiujące to schorzenie złogi IgA w co najmniej 7 wzorach) oraz oznaczenie surowiczych przeciwciał IgA techniką ELISA z jednym substratem do wyboru z zakresu transglutaminaza tkankowa (tTG) eTG nonapeptydy gliadyny (npG) neoepitopy gliadyna-tTG (neo-tTG) Owo postępowanie można uzupełnić o badanie histologiczne H+E wycinka ze skoacutery wykwitowej i badanie haplotypu HLA DQ2DQ8 u chorych z niejednoznacznym obrazem kliniczno-pracownianym
DH postępowanie lecznicze
Standardem terapeutycznym w DH czyli generalnie postępowaniem terapeutycznym z wyboru powinno natomiast być postępowanie dwuskładnikowe czyli powiązanie leczenia farmakologicznego kluczowym dapsonem i dietetycznego dietą bezglutenową w indywidualizowanych kombinacjach W postępowaniu leczniczym trzeba też uwzględnić całość problemoacutew zdrowotnych chorego
ACTA DERMATO-VENEREOLOGICA REVIEWERacuteS COMMENTS TO THE AUTHOR(S) Re Manuscript 114366 Authors Pasternack et al Title Quality of life and gastrointestinal symptoms in long-term g The authors analysed the HRQoL in DH patients on gluten free diet The topic is interesting however the study design is questionable First af all dermatitis herpetiformis is not a cutaneous manifestation of coeliac disease but it is rather a cutaneous disease associated with coeliac disease Furthermore the healthy group is poorly characterized (eg concomitant diseases are not mentioned at all eg Diabetes arterial hypertension) No comparison was performed regarding the age and gender distribution between DH patients and controls As there are differences within the DH patients regarding males and females a very low proportion of men in control group is an important bias as it seems that gender may be relevant cofactor In addition I would rather expect comparison between DH menhealthy men and DH womenhealthy women rather than between DH menDH women as the HRQOL in DH patients has been shown to be similar to controls The authors claimed that having ongoing skin symptoms at the time of the study had no influence on GSRS PGWB or SF-36 scores and the data are not shown In my opinion it is very probable that lack of significance was related to very small number of patients in the group of active skin lesions I would also expect from the authors to provide the information about concomitant gastrointestinal symptoms at the time of DH diagnosis It is probable that many of these patients never had clinically relevant symptoms of coeliac disease and thus GSRS would rather assess the effect of gluten-free diet on gastrointestinal symptoms instead of the relevance of coeliac disease symptomatology
Opryszczkowate zapalenie skoacutery jest
schorzeniem skoacuternym
bull nozologia DH jest zwodnicza dla wspoacutełczesnej społeczności
zwłaszcza niedermatologicznej
(opryszczkopodobne zapalenie skoacutery)
bull kontinuum autoimmunizacji i (auto)zapalenia
bull kluczowymi w skoacuternej patologii jawią się eTG i neutrofil
(uchwycenie zjawisk skoacuternych jak najbardziej DH-specyficznych)
bull DH to zapewne choroba skoacuterna z towarzyszącą nadwrażliwością na gluten
nieporozumienia
bull dapson na import docelowy
bull okolica łokciowa
bull pośladek jako miejsce wykonania DIFf
bull
foto Zbyszek KaczmarekGazeta Polska
Cutaneous expression of neutrophil elastase in relation
to IgA antibodies to nonapeptides of gliadin and
tissue transglutaminase in dermatitis
herpetiformis
Results
NE (top left) deposits in immunohistochemistry in
lesional skin in a male patient with DH
(immunoperoxidase staining on paraffin embedded
sections original magnification x200)
Intensity of NE (bottom left) deposits processed
with digital microscopic image analysis
superimposed on NE deposits
in immunohistochemistry in lesional skin in
this patient
Intensity of NE (top right) deposits processed with
digital microscopic image analysis in lesional skin in
this patient
Conclusions
bull Thus it seems that the production of IgA npG takes place in a coordinated way with the production of IgA tTG when patients show cutaneous lesions of DH
bull Nevertheless it is hypothesized that IgA npG and IgA tTG regardless of the issue of their diagnostic significance have lesser importance as far as cutaneous pathology of human DH mediated by DEJ-degrading NE released from IgA autoimmunity-activated neutrophils is concerned
Consistently with the autoimmune
origin of DH functional classification
of the differentially expressed genes
(DEGs) indicates a B- and T-cell
immune response (LAG3 TRAF5
DPP4 and NT5E) In addition gene
modulation provides evidence for a
local inflammatory response (IL8
PTGFR FSTL1 IFI16 BDKRD2
and NAMPT) with concomitant
leukocyte recruitment (CCL5
ENPP2) endothelial cell activation
and neutrophil extravasation (SELL
SELE) DEGs also indicate
overproduction of matrix proteases
(MMP9 ADAM9 and ADAM19) and
proteolytic enzymes (CTSG ELA2
CPA3 TPSB2 and CMA1) that may
contribute to epidermal splitting and
blister formation
In conclusion our data add DH
plaque psoriasis and
psoriatic arthritis to the growing
list of disorders associated
with Ig deregulation where the
enhancer HS12-A may be
involved
The incubation with Ni-Ti heat-
activated (T3) or Ni-Ti super-elastic
(T4) and with Ni-Cr-Co (T2) alloys
produced respectively 25-fold and 8-
fold increases in IL-6 release
compared with control cultures
Transglutaminase activity was
significantly increased in cells
exposed to T3 and T4 alloys (about
170 of control p lt 005) where it
was mainly localized close to inner
part of cell membrane The exposure
to T3 and T4 specimens significantly
up-regulated also tTG expression
compared with control cultures
These data first show an association
between IL-6 release and tissue
transglutaminase increases
suggesting that TGase-mediated
reactions may play a major role in
periodontal inflammation
pp 178-9
DH patomechanizm
Uważam że należy postrzegać DH jako chorobę skoacuterną z drugorzędnym udziałem patologii jelitowej
Sądzę że w skoacuternej patogenezie tej dermatozy wspoacutełgrają wzajemnie zapętlone zjawiska autoimmunizacji zależne od kluczowego autoantygenu ndash enzymu transglutaminazy naskoacuterkowej (eTG) przemieszczonej być może w wyniku mikrourazoacutew i drapania do skoacutery właściwej w bliskości połączenia skoacuterno-naskoacuterkowego (dermal-epidermal junction DEJ) z wyższych warstw naskoacuterka gdzie ma ona znaczenie fizjologiczne jako bdquoklej biologicznyrdquo (jeden z elementoacutew bdquobariery naskoacuterkowejrdquobdquokoperty rogowejrdquo) oraz (auto)zapalenia zależnego od uczynnionych neutrofiloacutew uwalniających elastazę neutrofiloacutew (NE) trawiącą DEJ z wytworzeniem rozwarstwienia w przestrzeni lamina lucida
DH postępowanie diagnostyczne
Standardem diagnostyki roacuteżnicowej DH powinno być postępowanie troacutejskładnikowe oparte o badanie kliniczne (co i gdzie)(stereotypowym chorym będzie młodzieniec lub młody mężczyzna) bezpośrednie badanie immunofluorescencyjne (DIF)skoacutery klinicznie niezmienionej z otoczenia wykwitoacutew analogicznie do pozostałych autoimmunizacyjnych dermatoz pęcherzowych (ujawnia definiujące to schorzenie złogi IgA w co najmniej 7 wzorach) oraz oznaczenie surowiczych przeciwciał IgA techniką ELISA z jednym substratem do wyboru z zakresu transglutaminaza tkankowa (tTG) eTG nonapeptydy gliadyny (npG) neoepitopy gliadyna-tTG (neo-tTG) Owo postępowanie można uzupełnić o badanie histologiczne H+E wycinka ze skoacutery wykwitowej i badanie haplotypu HLA DQ2DQ8 u chorych z niejednoznacznym obrazem kliniczno-pracownianym
DH postępowanie lecznicze
Standardem terapeutycznym w DH czyli generalnie postępowaniem terapeutycznym z wyboru powinno natomiast być postępowanie dwuskładnikowe czyli powiązanie leczenia farmakologicznego kluczowym dapsonem i dietetycznego dietą bezglutenową w indywidualizowanych kombinacjach W postępowaniu leczniczym trzeba też uwzględnić całość problemoacutew zdrowotnych chorego
ACTA DERMATO-VENEREOLOGICA REVIEWERacuteS COMMENTS TO THE AUTHOR(S) Re Manuscript 114366 Authors Pasternack et al Title Quality of life and gastrointestinal symptoms in long-term g The authors analysed the HRQoL in DH patients on gluten free diet The topic is interesting however the study design is questionable First af all dermatitis herpetiformis is not a cutaneous manifestation of coeliac disease but it is rather a cutaneous disease associated with coeliac disease Furthermore the healthy group is poorly characterized (eg concomitant diseases are not mentioned at all eg Diabetes arterial hypertension) No comparison was performed regarding the age and gender distribution between DH patients and controls As there are differences within the DH patients regarding males and females a very low proportion of men in control group is an important bias as it seems that gender may be relevant cofactor In addition I would rather expect comparison between DH menhealthy men and DH womenhealthy women rather than between DH menDH women as the HRQOL in DH patients has been shown to be similar to controls The authors claimed that having ongoing skin symptoms at the time of the study had no influence on GSRS PGWB or SF-36 scores and the data are not shown In my opinion it is very probable that lack of significance was related to very small number of patients in the group of active skin lesions I would also expect from the authors to provide the information about concomitant gastrointestinal symptoms at the time of DH diagnosis It is probable that many of these patients never had clinically relevant symptoms of coeliac disease and thus GSRS would rather assess the effect of gluten-free diet on gastrointestinal symptoms instead of the relevance of coeliac disease symptomatology
Opryszczkowate zapalenie skoacutery jest
schorzeniem skoacuternym
bull nozologia DH jest zwodnicza dla wspoacutełczesnej społeczności
zwłaszcza niedermatologicznej
(opryszczkopodobne zapalenie skoacutery)
bull kontinuum autoimmunizacji i (auto)zapalenia
bull kluczowymi w skoacuternej patologii jawią się eTG i neutrofil
(uchwycenie zjawisk skoacuternych jak najbardziej DH-specyficznych)
bull DH to zapewne choroba skoacuterna z towarzyszącą nadwrażliwością na gluten
nieporozumienia
bull dapson na import docelowy
bull okolica łokciowa
bull pośladek jako miejsce wykonania DIFf
bull
foto Zbyszek KaczmarekGazeta Polska
Results
NE (top left) deposits in immunohistochemistry in
lesional skin in a male patient with DH
(immunoperoxidase staining on paraffin embedded
sections original magnification x200)
Intensity of NE (bottom left) deposits processed
with digital microscopic image analysis
superimposed on NE deposits
in immunohistochemistry in lesional skin in
this patient
Intensity of NE (top right) deposits processed with
digital microscopic image analysis in lesional skin in
this patient
Conclusions
bull Thus it seems that the production of IgA npG takes place in a coordinated way with the production of IgA tTG when patients show cutaneous lesions of DH
bull Nevertheless it is hypothesized that IgA npG and IgA tTG regardless of the issue of their diagnostic significance have lesser importance as far as cutaneous pathology of human DH mediated by DEJ-degrading NE released from IgA autoimmunity-activated neutrophils is concerned
Consistently with the autoimmune
origin of DH functional classification
of the differentially expressed genes
(DEGs) indicates a B- and T-cell
immune response (LAG3 TRAF5
DPP4 and NT5E) In addition gene
modulation provides evidence for a
local inflammatory response (IL8
PTGFR FSTL1 IFI16 BDKRD2
and NAMPT) with concomitant
leukocyte recruitment (CCL5
ENPP2) endothelial cell activation
and neutrophil extravasation (SELL
SELE) DEGs also indicate
overproduction of matrix proteases
(MMP9 ADAM9 and ADAM19) and
proteolytic enzymes (CTSG ELA2
CPA3 TPSB2 and CMA1) that may
contribute to epidermal splitting and
blister formation
In conclusion our data add DH
plaque psoriasis and
psoriatic arthritis to the growing
list of disorders associated
with Ig deregulation where the
enhancer HS12-A may be
involved
The incubation with Ni-Ti heat-
activated (T3) or Ni-Ti super-elastic
(T4) and with Ni-Cr-Co (T2) alloys
produced respectively 25-fold and 8-
fold increases in IL-6 release
compared with control cultures
Transglutaminase activity was
significantly increased in cells
exposed to T3 and T4 alloys (about
170 of control p lt 005) where it
was mainly localized close to inner
part of cell membrane The exposure
to T3 and T4 specimens significantly
up-regulated also tTG expression
compared with control cultures
These data first show an association
between IL-6 release and tissue
transglutaminase increases
suggesting that TGase-mediated
reactions may play a major role in
periodontal inflammation
pp 178-9
DH patomechanizm
Uważam że należy postrzegać DH jako chorobę skoacuterną z drugorzędnym udziałem patologii jelitowej
Sądzę że w skoacuternej patogenezie tej dermatozy wspoacutełgrają wzajemnie zapętlone zjawiska autoimmunizacji zależne od kluczowego autoantygenu ndash enzymu transglutaminazy naskoacuterkowej (eTG) przemieszczonej być może w wyniku mikrourazoacutew i drapania do skoacutery właściwej w bliskości połączenia skoacuterno-naskoacuterkowego (dermal-epidermal junction DEJ) z wyższych warstw naskoacuterka gdzie ma ona znaczenie fizjologiczne jako bdquoklej biologicznyrdquo (jeden z elementoacutew bdquobariery naskoacuterkowejrdquobdquokoperty rogowejrdquo) oraz (auto)zapalenia zależnego od uczynnionych neutrofiloacutew uwalniających elastazę neutrofiloacutew (NE) trawiącą DEJ z wytworzeniem rozwarstwienia w przestrzeni lamina lucida
DH postępowanie diagnostyczne
Standardem diagnostyki roacuteżnicowej DH powinno być postępowanie troacutejskładnikowe oparte o badanie kliniczne (co i gdzie)(stereotypowym chorym będzie młodzieniec lub młody mężczyzna) bezpośrednie badanie immunofluorescencyjne (DIF)skoacutery klinicznie niezmienionej z otoczenia wykwitoacutew analogicznie do pozostałych autoimmunizacyjnych dermatoz pęcherzowych (ujawnia definiujące to schorzenie złogi IgA w co najmniej 7 wzorach) oraz oznaczenie surowiczych przeciwciał IgA techniką ELISA z jednym substratem do wyboru z zakresu transglutaminaza tkankowa (tTG) eTG nonapeptydy gliadyny (npG) neoepitopy gliadyna-tTG (neo-tTG) Owo postępowanie można uzupełnić o badanie histologiczne H+E wycinka ze skoacutery wykwitowej i badanie haplotypu HLA DQ2DQ8 u chorych z niejednoznacznym obrazem kliniczno-pracownianym
DH postępowanie lecznicze
Standardem terapeutycznym w DH czyli generalnie postępowaniem terapeutycznym z wyboru powinno natomiast być postępowanie dwuskładnikowe czyli powiązanie leczenia farmakologicznego kluczowym dapsonem i dietetycznego dietą bezglutenową w indywidualizowanych kombinacjach W postępowaniu leczniczym trzeba też uwzględnić całość problemoacutew zdrowotnych chorego
ACTA DERMATO-VENEREOLOGICA REVIEWERacuteS COMMENTS TO THE AUTHOR(S) Re Manuscript 114366 Authors Pasternack et al Title Quality of life and gastrointestinal symptoms in long-term g The authors analysed the HRQoL in DH patients on gluten free diet The topic is interesting however the study design is questionable First af all dermatitis herpetiformis is not a cutaneous manifestation of coeliac disease but it is rather a cutaneous disease associated with coeliac disease Furthermore the healthy group is poorly characterized (eg concomitant diseases are not mentioned at all eg Diabetes arterial hypertension) No comparison was performed regarding the age and gender distribution between DH patients and controls As there are differences within the DH patients regarding males and females a very low proportion of men in control group is an important bias as it seems that gender may be relevant cofactor In addition I would rather expect comparison between DH menhealthy men and DH womenhealthy women rather than between DH menDH women as the HRQOL in DH patients has been shown to be similar to controls The authors claimed that having ongoing skin symptoms at the time of the study had no influence on GSRS PGWB or SF-36 scores and the data are not shown In my opinion it is very probable that lack of significance was related to very small number of patients in the group of active skin lesions I would also expect from the authors to provide the information about concomitant gastrointestinal symptoms at the time of DH diagnosis It is probable that many of these patients never had clinically relevant symptoms of coeliac disease and thus GSRS would rather assess the effect of gluten-free diet on gastrointestinal symptoms instead of the relevance of coeliac disease symptomatology
Opryszczkowate zapalenie skoacutery jest
schorzeniem skoacuternym
bull nozologia DH jest zwodnicza dla wspoacutełczesnej społeczności
zwłaszcza niedermatologicznej
(opryszczkopodobne zapalenie skoacutery)
bull kontinuum autoimmunizacji i (auto)zapalenia
bull kluczowymi w skoacuternej patologii jawią się eTG i neutrofil
(uchwycenie zjawisk skoacuternych jak najbardziej DH-specyficznych)
bull DH to zapewne choroba skoacuterna z towarzyszącą nadwrażliwością na gluten
nieporozumienia
bull dapson na import docelowy
bull okolica łokciowa
bull pośladek jako miejsce wykonania DIFf
bull
foto Zbyszek KaczmarekGazeta Polska
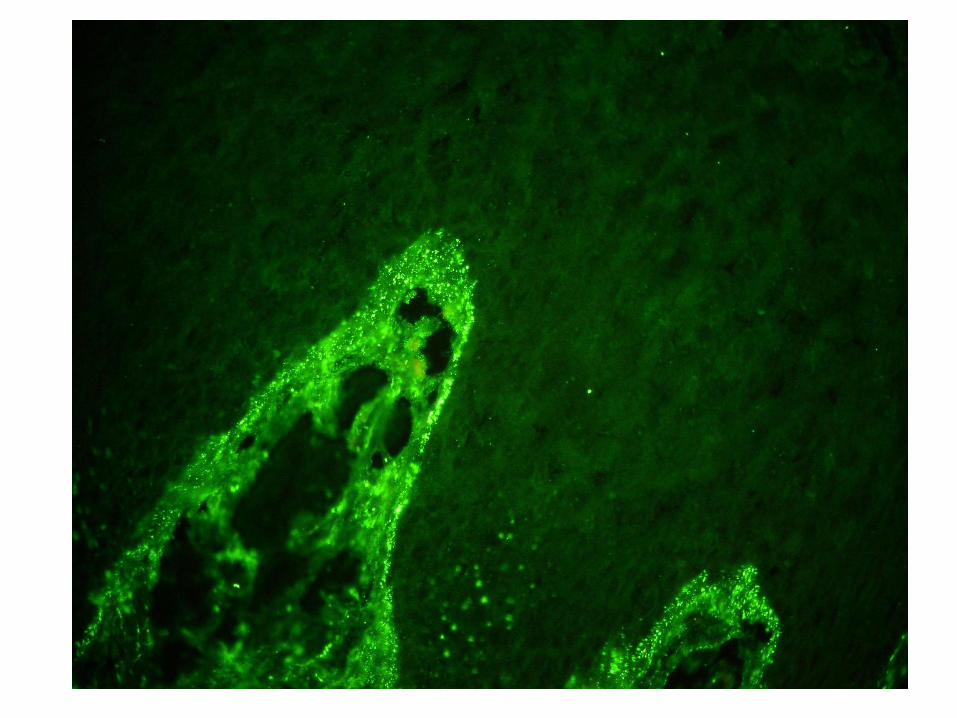
Conclusions
bull Thus it seems that the production of IgA npG takes place in a coordinated way with the production of IgA tTG when patients show cutaneous lesions of DH
bull Nevertheless it is hypothesized that IgA npG and IgA tTG regardless of the issue of their diagnostic significance have lesser importance as far as cutaneous pathology of human DH mediated by DEJ-degrading NE released from IgA autoimmunity-activated neutrophils is concerned
Consistently with the autoimmune
origin of DH functional classification
of the differentially expressed genes
(DEGs) indicates a B- and T-cell
immune response (LAG3 TRAF5
DPP4 and NT5E) In addition gene
modulation provides evidence for a
local inflammatory response (IL8
PTGFR FSTL1 IFI16 BDKRD2
and NAMPT) with concomitant
leukocyte recruitment (CCL5
ENPP2) endothelial cell activation
and neutrophil extravasation (SELL
SELE) DEGs also indicate
overproduction of matrix proteases
(MMP9 ADAM9 and ADAM19) and
proteolytic enzymes (CTSG ELA2
CPA3 TPSB2 and CMA1) that may
contribute to epidermal splitting and
blister formation
In conclusion our data add DH
plaque psoriasis and
psoriatic arthritis to the growing
list of disorders associated
with Ig deregulation where the
enhancer HS12-A may be
involved
The incubation with Ni-Ti heat-
activated (T3) or Ni-Ti super-elastic
(T4) and with Ni-Cr-Co (T2) alloys
produced respectively 25-fold and 8-
fold increases in IL-6 release
compared with control cultures
Transglutaminase activity was
significantly increased in cells
exposed to T3 and T4 alloys (about
170 of control p lt 005) where it
was mainly localized close to inner
part of cell membrane The exposure
to T3 and T4 specimens significantly
up-regulated also tTG expression
compared with control cultures
These data first show an association
between IL-6 release and tissue
transglutaminase increases
suggesting that TGase-mediated
reactions may play a major role in
periodontal inflammation
pp 178-9
DH patomechanizm
Uważam że należy postrzegać DH jako chorobę skoacuterną z drugorzędnym udziałem patologii jelitowej
Sądzę że w skoacuternej patogenezie tej dermatozy wspoacutełgrają wzajemnie zapętlone zjawiska autoimmunizacji zależne od kluczowego autoantygenu ndash enzymu transglutaminazy naskoacuterkowej (eTG) przemieszczonej być może w wyniku mikrourazoacutew i drapania do skoacutery właściwej w bliskości połączenia skoacuterno-naskoacuterkowego (dermal-epidermal junction DEJ) z wyższych warstw naskoacuterka gdzie ma ona znaczenie fizjologiczne jako bdquoklej biologicznyrdquo (jeden z elementoacutew bdquobariery naskoacuterkowejrdquobdquokoperty rogowejrdquo) oraz (auto)zapalenia zależnego od uczynnionych neutrofiloacutew uwalniających elastazę neutrofiloacutew (NE) trawiącą DEJ z wytworzeniem rozwarstwienia w przestrzeni lamina lucida
DH postępowanie diagnostyczne
Standardem diagnostyki roacuteżnicowej DH powinno być postępowanie troacutejskładnikowe oparte o badanie kliniczne (co i gdzie)(stereotypowym chorym będzie młodzieniec lub młody mężczyzna) bezpośrednie badanie immunofluorescencyjne (DIF)skoacutery klinicznie niezmienionej z otoczenia wykwitoacutew analogicznie do pozostałych autoimmunizacyjnych dermatoz pęcherzowych (ujawnia definiujące to schorzenie złogi IgA w co najmniej 7 wzorach) oraz oznaczenie surowiczych przeciwciał IgA techniką ELISA z jednym substratem do wyboru z zakresu transglutaminaza tkankowa (tTG) eTG nonapeptydy gliadyny (npG) neoepitopy gliadyna-tTG (neo-tTG) Owo postępowanie można uzupełnić o badanie histologiczne H+E wycinka ze skoacutery wykwitowej i badanie haplotypu HLA DQ2DQ8 u chorych z niejednoznacznym obrazem kliniczno-pracownianym
DH postępowanie lecznicze
Standardem terapeutycznym w DH czyli generalnie postępowaniem terapeutycznym z wyboru powinno natomiast być postępowanie dwuskładnikowe czyli powiązanie leczenia farmakologicznego kluczowym dapsonem i dietetycznego dietą bezglutenową w indywidualizowanych kombinacjach W postępowaniu leczniczym trzeba też uwzględnić całość problemoacutew zdrowotnych chorego
ACTA DERMATO-VENEREOLOGICA REVIEWERacuteS COMMENTS TO THE AUTHOR(S) Re Manuscript 114366 Authors Pasternack et al Title Quality of life and gastrointestinal symptoms in long-term g The authors analysed the HRQoL in DH patients on gluten free diet The topic is interesting however the study design is questionable First af all dermatitis herpetiformis is not a cutaneous manifestation of coeliac disease but it is rather a cutaneous disease associated with coeliac disease Furthermore the healthy group is poorly characterized (eg concomitant diseases are not mentioned at all eg Diabetes arterial hypertension) No comparison was performed regarding the age and gender distribution between DH patients and controls As there are differences within the DH patients regarding males and females a very low proportion of men in control group is an important bias as it seems that gender may be relevant cofactor In addition I would rather expect comparison between DH menhealthy men and DH womenhealthy women rather than between DH menDH women as the HRQOL in DH patients has been shown to be similar to controls The authors claimed that having ongoing skin symptoms at the time of the study had no influence on GSRS PGWB or SF-36 scores and the data are not shown In my opinion it is very probable that lack of significance was related to very small number of patients in the group of active skin lesions I would also expect from the authors to provide the information about concomitant gastrointestinal symptoms at the time of DH diagnosis It is probable that many of these patients never had clinically relevant symptoms of coeliac disease and thus GSRS would rather assess the effect of gluten-free diet on gastrointestinal symptoms instead of the relevance of coeliac disease symptomatology
Opryszczkowate zapalenie skoacutery jest
schorzeniem skoacuternym
bull nozologia DH jest zwodnicza dla wspoacutełczesnej społeczności
zwłaszcza niedermatologicznej
(opryszczkopodobne zapalenie skoacutery)
bull kontinuum autoimmunizacji i (auto)zapalenia
bull kluczowymi w skoacuternej patologii jawią się eTG i neutrofil
(uchwycenie zjawisk skoacuternych jak najbardziej DH-specyficznych)
bull DH to zapewne choroba skoacuterna z towarzyszącą nadwrażliwością na gluten
nieporozumienia
bull dapson na import docelowy
bull okolica łokciowa
bull pośladek jako miejsce wykonania DIFf
bull
foto Zbyszek KaczmarekGazeta Polska
Consistently with the autoimmune
origin of DH functional classification
of the differentially expressed genes
(DEGs) indicates a B- and T-cell
immune response (LAG3 TRAF5
DPP4 and NT5E) In addition gene
modulation provides evidence for a
local inflammatory response (IL8
PTGFR FSTL1 IFI16 BDKRD2
and NAMPT) with concomitant
leukocyte recruitment (CCL5
ENPP2) endothelial cell activation
and neutrophil extravasation (SELL
SELE) DEGs also indicate
overproduction of matrix proteases
(MMP9 ADAM9 and ADAM19) and
proteolytic enzymes (CTSG ELA2
CPA3 TPSB2 and CMA1) that may
contribute to epidermal splitting and
blister formation
In conclusion our data add DH
plaque psoriasis and
psoriatic arthritis to the growing
list of disorders associated
with Ig deregulation where the
enhancer HS12-A may be
involved
The incubation with Ni-Ti heat-
activated (T3) or Ni-Ti super-elastic
(T4) and with Ni-Cr-Co (T2) alloys
produced respectively 25-fold and 8-
fold increases in IL-6 release
compared with control cultures
Transglutaminase activity was
significantly increased in cells
exposed to T3 and T4 alloys (about
170 of control p lt 005) where it
was mainly localized close to inner
part of cell membrane The exposure
to T3 and T4 specimens significantly
up-regulated also tTG expression
compared with control cultures
These data first show an association
between IL-6 release and tissue
transglutaminase increases
suggesting that TGase-mediated
reactions may play a major role in
periodontal inflammation
pp 178-9
DH patomechanizm
Uważam że należy postrzegać DH jako chorobę skoacuterną z drugorzędnym udziałem patologii jelitowej
Sądzę że w skoacuternej patogenezie tej dermatozy wspoacutełgrają wzajemnie zapętlone zjawiska autoimmunizacji zależne od kluczowego autoantygenu ndash enzymu transglutaminazy naskoacuterkowej (eTG) przemieszczonej być może w wyniku mikrourazoacutew i drapania do skoacutery właściwej w bliskości połączenia skoacuterno-naskoacuterkowego (dermal-epidermal junction DEJ) z wyższych warstw naskoacuterka gdzie ma ona znaczenie fizjologiczne jako bdquoklej biologicznyrdquo (jeden z elementoacutew bdquobariery naskoacuterkowejrdquobdquokoperty rogowejrdquo) oraz (auto)zapalenia zależnego od uczynnionych neutrofiloacutew uwalniających elastazę neutrofiloacutew (NE) trawiącą DEJ z wytworzeniem rozwarstwienia w przestrzeni lamina lucida
DH postępowanie diagnostyczne
Standardem diagnostyki roacuteżnicowej DH powinno być postępowanie troacutejskładnikowe oparte o badanie kliniczne (co i gdzie)(stereotypowym chorym będzie młodzieniec lub młody mężczyzna) bezpośrednie badanie immunofluorescencyjne (DIF)skoacutery klinicznie niezmienionej z otoczenia wykwitoacutew analogicznie do pozostałych autoimmunizacyjnych dermatoz pęcherzowych (ujawnia definiujące to schorzenie złogi IgA w co najmniej 7 wzorach) oraz oznaczenie surowiczych przeciwciał IgA techniką ELISA z jednym substratem do wyboru z zakresu transglutaminaza tkankowa (tTG) eTG nonapeptydy gliadyny (npG) neoepitopy gliadyna-tTG (neo-tTG) Owo postępowanie można uzupełnić o badanie histologiczne H+E wycinka ze skoacutery wykwitowej i badanie haplotypu HLA DQ2DQ8 u chorych z niejednoznacznym obrazem kliniczno-pracownianym
DH postępowanie lecznicze
Standardem terapeutycznym w DH czyli generalnie postępowaniem terapeutycznym z wyboru powinno natomiast być postępowanie dwuskładnikowe czyli powiązanie leczenia farmakologicznego kluczowym dapsonem i dietetycznego dietą bezglutenową w indywidualizowanych kombinacjach W postępowaniu leczniczym trzeba też uwzględnić całość problemoacutew zdrowotnych chorego
ACTA DERMATO-VENEREOLOGICA REVIEWERacuteS COMMENTS TO THE AUTHOR(S) Re Manuscript 114366 Authors Pasternack et al Title Quality of life and gastrointestinal symptoms in long-term g The authors analysed the HRQoL in DH patients on gluten free diet The topic is interesting however the study design is questionable First af all dermatitis herpetiformis is not a cutaneous manifestation of coeliac disease but it is rather a cutaneous disease associated with coeliac disease Furthermore the healthy group is poorly characterized (eg concomitant diseases are not mentioned at all eg Diabetes arterial hypertension) No comparison was performed regarding the age and gender distribution between DH patients and controls As there are differences within the DH patients regarding males and females a very low proportion of men in control group is an important bias as it seems that gender may be relevant cofactor In addition I would rather expect comparison between DH menhealthy men and DH womenhealthy women rather than between DH menDH women as the HRQOL in DH patients has been shown to be similar to controls The authors claimed that having ongoing skin symptoms at the time of the study had no influence on GSRS PGWB or SF-36 scores and the data are not shown In my opinion it is very probable that lack of significance was related to very small number of patients in the group of active skin lesions I would also expect from the authors to provide the information about concomitant gastrointestinal symptoms at the time of DH diagnosis It is probable that many of these patients never had clinically relevant symptoms of coeliac disease and thus GSRS would rather assess the effect of gluten-free diet on gastrointestinal symptoms instead of the relevance of coeliac disease symptomatology
Opryszczkowate zapalenie skoacutery jest
schorzeniem skoacuternym
bull nozologia DH jest zwodnicza dla wspoacutełczesnej społeczności
zwłaszcza niedermatologicznej
(opryszczkopodobne zapalenie skoacutery)
bull kontinuum autoimmunizacji i (auto)zapalenia
bull kluczowymi w skoacuternej patologii jawią się eTG i neutrofil
(uchwycenie zjawisk skoacuternych jak najbardziej DH-specyficznych)
bull DH to zapewne choroba skoacuterna z towarzyszącą nadwrażliwością na gluten
nieporozumienia
bull dapson na import docelowy
bull okolica łokciowa
bull pośladek jako miejsce wykonania DIFf
bull
foto Zbyszek KaczmarekGazeta Polska
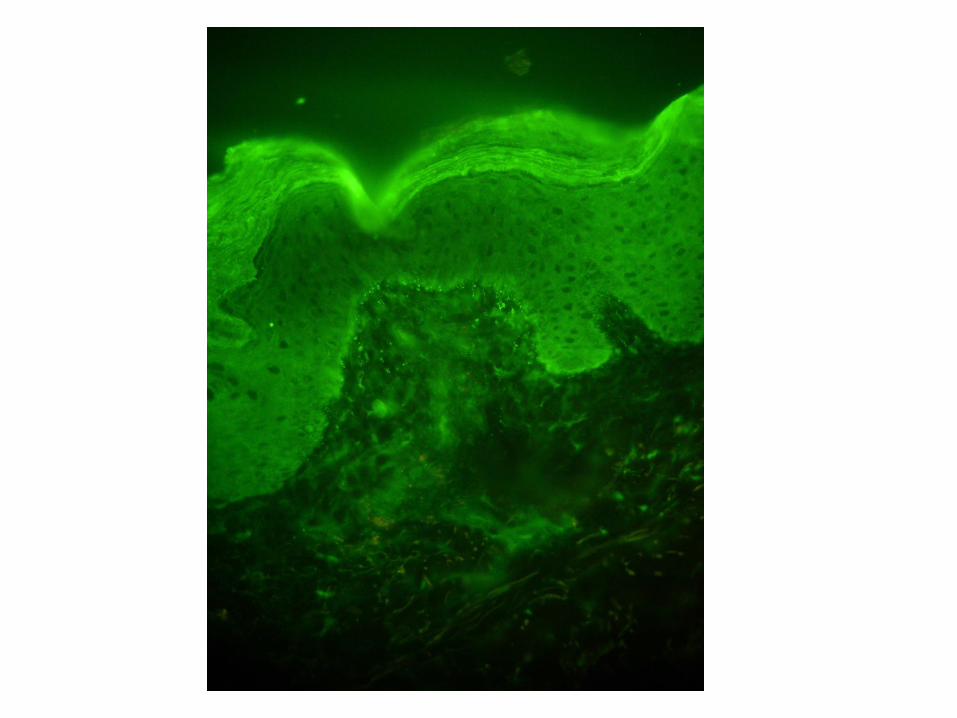
In conclusion our data add DH
plaque psoriasis and
psoriatic arthritis to the growing
list of disorders associated
with Ig deregulation where the
enhancer HS12-A may be
involved
The incubation with Ni-Ti heat-
activated (T3) or Ni-Ti super-elastic
(T4) and with Ni-Cr-Co (T2) alloys
produced respectively 25-fold and 8-
fold increases in IL-6 release
compared with control cultures
Transglutaminase activity was
significantly increased in cells
exposed to T3 and T4 alloys (about
170 of control p lt 005) where it
was mainly localized close to inner
part of cell membrane The exposure
to T3 and T4 specimens significantly
up-regulated also tTG expression
compared with control cultures
These data first show an association
between IL-6 release and tissue
transglutaminase increases
suggesting that TGase-mediated
reactions may play a major role in
periodontal inflammation
pp 178-9
DH patomechanizm
Uważam że należy postrzegać DH jako chorobę skoacuterną z drugorzędnym udziałem patologii jelitowej
Sądzę że w skoacuternej patogenezie tej dermatozy wspoacutełgrają wzajemnie zapętlone zjawiska autoimmunizacji zależne od kluczowego autoantygenu ndash enzymu transglutaminazy naskoacuterkowej (eTG) przemieszczonej być może w wyniku mikrourazoacutew i drapania do skoacutery właściwej w bliskości połączenia skoacuterno-naskoacuterkowego (dermal-epidermal junction DEJ) z wyższych warstw naskoacuterka gdzie ma ona znaczenie fizjologiczne jako bdquoklej biologicznyrdquo (jeden z elementoacutew bdquobariery naskoacuterkowejrdquobdquokoperty rogowejrdquo) oraz (auto)zapalenia zależnego od uczynnionych neutrofiloacutew uwalniających elastazę neutrofiloacutew (NE) trawiącą DEJ z wytworzeniem rozwarstwienia w przestrzeni lamina lucida
DH postępowanie diagnostyczne
Standardem diagnostyki roacuteżnicowej DH powinno być postępowanie troacutejskładnikowe oparte o badanie kliniczne (co i gdzie)(stereotypowym chorym będzie młodzieniec lub młody mężczyzna) bezpośrednie badanie immunofluorescencyjne (DIF)skoacutery klinicznie niezmienionej z otoczenia wykwitoacutew analogicznie do pozostałych autoimmunizacyjnych dermatoz pęcherzowych (ujawnia definiujące to schorzenie złogi IgA w co najmniej 7 wzorach) oraz oznaczenie surowiczych przeciwciał IgA techniką ELISA z jednym substratem do wyboru z zakresu transglutaminaza tkankowa (tTG) eTG nonapeptydy gliadyny (npG) neoepitopy gliadyna-tTG (neo-tTG) Owo postępowanie można uzupełnić o badanie histologiczne H+E wycinka ze skoacutery wykwitowej i badanie haplotypu HLA DQ2DQ8 u chorych z niejednoznacznym obrazem kliniczno-pracownianym
DH postępowanie lecznicze
Standardem terapeutycznym w DH czyli generalnie postępowaniem terapeutycznym z wyboru powinno natomiast być postępowanie dwuskładnikowe czyli powiązanie leczenia farmakologicznego kluczowym dapsonem i dietetycznego dietą bezglutenową w indywidualizowanych kombinacjach W postępowaniu leczniczym trzeba też uwzględnić całość problemoacutew zdrowotnych chorego
ACTA DERMATO-VENEREOLOGICA REVIEWERacuteS COMMENTS TO THE AUTHOR(S) Re Manuscript 114366 Authors Pasternack et al Title Quality of life and gastrointestinal symptoms in long-term g The authors analysed the HRQoL in DH patients on gluten free diet The topic is interesting however the study design is questionable First af all dermatitis herpetiformis is not a cutaneous manifestation of coeliac disease but it is rather a cutaneous disease associated with coeliac disease Furthermore the healthy group is poorly characterized (eg concomitant diseases are not mentioned at all eg Diabetes arterial hypertension) No comparison was performed regarding the age and gender distribution between DH patients and controls As there are differences within the DH patients regarding males and females a very low proportion of men in control group is an important bias as it seems that gender may be relevant cofactor In addition I would rather expect comparison between DH menhealthy men and DH womenhealthy women rather than between DH menDH women as the HRQOL in DH patients has been shown to be similar to controls The authors claimed that having ongoing skin symptoms at the time of the study had no influence on GSRS PGWB or SF-36 scores and the data are not shown In my opinion it is very probable that lack of significance was related to very small number of patients in the group of active skin lesions I would also expect from the authors to provide the information about concomitant gastrointestinal symptoms at the time of DH diagnosis It is probable that many of these patients never had clinically relevant symptoms of coeliac disease and thus GSRS would rather assess the effect of gluten-free diet on gastrointestinal symptoms instead of the relevance of coeliac disease symptomatology
Opryszczkowate zapalenie skoacutery jest
schorzeniem skoacuternym
bull nozologia DH jest zwodnicza dla wspoacutełczesnej społeczności
zwłaszcza niedermatologicznej
(opryszczkopodobne zapalenie skoacutery)
bull kontinuum autoimmunizacji i (auto)zapalenia
bull kluczowymi w skoacuternej patologii jawią się eTG i neutrofil
(uchwycenie zjawisk skoacuternych jak najbardziej DH-specyficznych)
bull DH to zapewne choroba skoacuterna z towarzyszącą nadwrażliwością na gluten
nieporozumienia
bull dapson na import docelowy
bull okolica łokciowa
bull pośladek jako miejsce wykonania DIFf
bull
foto Zbyszek KaczmarekGazeta Polska
The incubation with Ni-Ti heat-
activated (T3) or Ni-Ti super-elastic
(T4) and with Ni-Cr-Co (T2) alloys
produced respectively 25-fold and 8-
fold increases in IL-6 release
compared with control cultures
Transglutaminase activity was
significantly increased in cells
exposed to T3 and T4 alloys (about
170 of control p lt 005) where it
was mainly localized close to inner
part of cell membrane The exposure
to T3 and T4 specimens significantly
up-regulated also tTG expression
compared with control cultures
These data first show an association
between IL-6 release and tissue
transglutaminase increases
suggesting that TGase-mediated
reactions may play a major role in
periodontal inflammation
pp 178-9
DH patomechanizm
Uważam że należy postrzegać DH jako chorobę skoacuterną z drugorzędnym udziałem patologii jelitowej
Sądzę że w skoacuternej patogenezie tej dermatozy wspoacutełgrają wzajemnie zapętlone zjawiska autoimmunizacji zależne od kluczowego autoantygenu ndash enzymu transglutaminazy naskoacuterkowej (eTG) przemieszczonej być może w wyniku mikrourazoacutew i drapania do skoacutery właściwej w bliskości połączenia skoacuterno-naskoacuterkowego (dermal-epidermal junction DEJ) z wyższych warstw naskoacuterka gdzie ma ona znaczenie fizjologiczne jako bdquoklej biologicznyrdquo (jeden z elementoacutew bdquobariery naskoacuterkowejrdquobdquokoperty rogowejrdquo) oraz (auto)zapalenia zależnego od uczynnionych neutrofiloacutew uwalniających elastazę neutrofiloacutew (NE) trawiącą DEJ z wytworzeniem rozwarstwienia w przestrzeni lamina lucida
DH postępowanie diagnostyczne
Standardem diagnostyki roacuteżnicowej DH powinno być postępowanie troacutejskładnikowe oparte o badanie kliniczne (co i gdzie)(stereotypowym chorym będzie młodzieniec lub młody mężczyzna) bezpośrednie badanie immunofluorescencyjne (DIF)skoacutery klinicznie niezmienionej z otoczenia wykwitoacutew analogicznie do pozostałych autoimmunizacyjnych dermatoz pęcherzowych (ujawnia definiujące to schorzenie złogi IgA w co najmniej 7 wzorach) oraz oznaczenie surowiczych przeciwciał IgA techniką ELISA z jednym substratem do wyboru z zakresu transglutaminaza tkankowa (tTG) eTG nonapeptydy gliadyny (npG) neoepitopy gliadyna-tTG (neo-tTG) Owo postępowanie można uzupełnić o badanie histologiczne H+E wycinka ze skoacutery wykwitowej i badanie haplotypu HLA DQ2DQ8 u chorych z niejednoznacznym obrazem kliniczno-pracownianym
DH postępowanie lecznicze
Standardem terapeutycznym w DH czyli generalnie postępowaniem terapeutycznym z wyboru powinno natomiast być postępowanie dwuskładnikowe czyli powiązanie leczenia farmakologicznego kluczowym dapsonem i dietetycznego dietą bezglutenową w indywidualizowanych kombinacjach W postępowaniu leczniczym trzeba też uwzględnić całość problemoacutew zdrowotnych chorego
ACTA DERMATO-VENEREOLOGICA REVIEWERacuteS COMMENTS TO THE AUTHOR(S) Re Manuscript 114366 Authors Pasternack et al Title Quality of life and gastrointestinal symptoms in long-term g The authors analysed the HRQoL in DH patients on gluten free diet The topic is interesting however the study design is questionable First af all dermatitis herpetiformis is not a cutaneous manifestation of coeliac disease but it is rather a cutaneous disease associated with coeliac disease Furthermore the healthy group is poorly characterized (eg concomitant diseases are not mentioned at all eg Diabetes arterial hypertension) No comparison was performed regarding the age and gender distribution between DH patients and controls As there are differences within the DH patients regarding males and females a very low proportion of men in control group is an important bias as it seems that gender may be relevant cofactor In addition I would rather expect comparison between DH menhealthy men and DH womenhealthy women rather than between DH menDH women as the HRQOL in DH patients has been shown to be similar to controls The authors claimed that having ongoing skin symptoms at the time of the study had no influence on GSRS PGWB or SF-36 scores and the data are not shown In my opinion it is very probable that lack of significance was related to very small number of patients in the group of active skin lesions I would also expect from the authors to provide the information about concomitant gastrointestinal symptoms at the time of DH diagnosis It is probable that many of these patients never had clinically relevant symptoms of coeliac disease and thus GSRS would rather assess the effect of gluten-free diet on gastrointestinal symptoms instead of the relevance of coeliac disease symptomatology
Opryszczkowate zapalenie skoacutery jest
schorzeniem skoacuternym
bull nozologia DH jest zwodnicza dla wspoacutełczesnej społeczności
zwłaszcza niedermatologicznej
(opryszczkopodobne zapalenie skoacutery)
bull kontinuum autoimmunizacji i (auto)zapalenia
bull kluczowymi w skoacuternej patologii jawią się eTG i neutrofil
(uchwycenie zjawisk skoacuternych jak najbardziej DH-specyficznych)
bull DH to zapewne choroba skoacuterna z towarzyszącą nadwrażliwością na gluten
nieporozumienia
bull dapson na import docelowy
bull okolica łokciowa
bull pośladek jako miejsce wykonania DIFf
bull
foto Zbyszek KaczmarekGazeta Polska
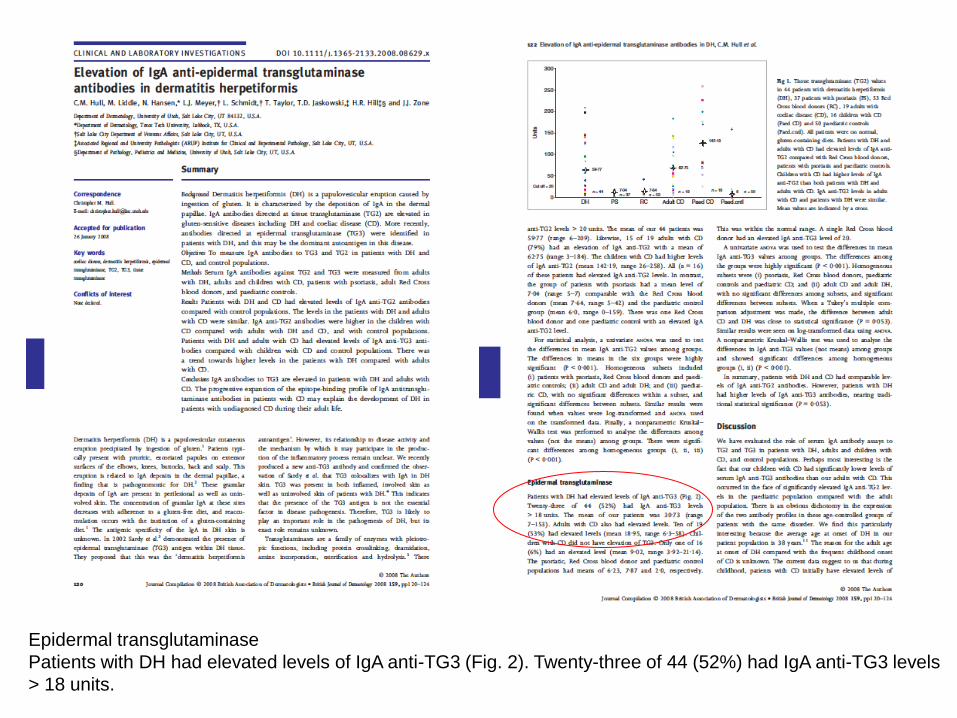
pp 178-9
DH patomechanizm
Uważam że należy postrzegać DH jako chorobę skoacuterną z drugorzędnym udziałem patologii jelitowej
Sądzę że w skoacuternej patogenezie tej dermatozy wspoacutełgrają wzajemnie zapętlone zjawiska autoimmunizacji zależne od kluczowego autoantygenu ndash enzymu transglutaminazy naskoacuterkowej (eTG) przemieszczonej być może w wyniku mikrourazoacutew i drapania do skoacutery właściwej w bliskości połączenia skoacuterno-naskoacuterkowego (dermal-epidermal junction DEJ) z wyższych warstw naskoacuterka gdzie ma ona znaczenie fizjologiczne jako bdquoklej biologicznyrdquo (jeden z elementoacutew bdquobariery naskoacuterkowejrdquobdquokoperty rogowejrdquo) oraz (auto)zapalenia zależnego od uczynnionych neutrofiloacutew uwalniających elastazę neutrofiloacutew (NE) trawiącą DEJ z wytworzeniem rozwarstwienia w przestrzeni lamina lucida
DH postępowanie diagnostyczne
Standardem diagnostyki roacuteżnicowej DH powinno być postępowanie troacutejskładnikowe oparte o badanie kliniczne (co i gdzie)(stereotypowym chorym będzie młodzieniec lub młody mężczyzna) bezpośrednie badanie immunofluorescencyjne (DIF)skoacutery klinicznie niezmienionej z otoczenia wykwitoacutew analogicznie do pozostałych autoimmunizacyjnych dermatoz pęcherzowych (ujawnia definiujące to schorzenie złogi IgA w co najmniej 7 wzorach) oraz oznaczenie surowiczych przeciwciał IgA techniką ELISA z jednym substratem do wyboru z zakresu transglutaminaza tkankowa (tTG) eTG nonapeptydy gliadyny (npG) neoepitopy gliadyna-tTG (neo-tTG) Owo postępowanie można uzupełnić o badanie histologiczne H+E wycinka ze skoacutery wykwitowej i badanie haplotypu HLA DQ2DQ8 u chorych z niejednoznacznym obrazem kliniczno-pracownianym
DH postępowanie lecznicze
Standardem terapeutycznym w DH czyli generalnie postępowaniem terapeutycznym z wyboru powinno natomiast być postępowanie dwuskładnikowe czyli powiązanie leczenia farmakologicznego kluczowym dapsonem i dietetycznego dietą bezglutenową w indywidualizowanych kombinacjach W postępowaniu leczniczym trzeba też uwzględnić całość problemoacutew zdrowotnych chorego
ACTA DERMATO-VENEREOLOGICA REVIEWERacuteS COMMENTS TO THE AUTHOR(S) Re Manuscript 114366 Authors Pasternack et al Title Quality of life and gastrointestinal symptoms in long-term g The authors analysed the HRQoL in DH patients on gluten free diet The topic is interesting however the study design is questionable First af all dermatitis herpetiformis is not a cutaneous manifestation of coeliac disease but it is rather a cutaneous disease associated with coeliac disease Furthermore the healthy group is poorly characterized (eg concomitant diseases are not mentioned at all eg Diabetes arterial hypertension) No comparison was performed regarding the age and gender distribution between DH patients and controls As there are differences within the DH patients regarding males and females a very low proportion of men in control group is an important bias as it seems that gender may be relevant cofactor In addition I would rather expect comparison between DH menhealthy men and DH womenhealthy women rather than between DH menDH women as the HRQOL in DH patients has been shown to be similar to controls The authors claimed that having ongoing skin symptoms at the time of the study had no influence on GSRS PGWB or SF-36 scores and the data are not shown In my opinion it is very probable that lack of significance was related to very small number of patients in the group of active skin lesions I would also expect from the authors to provide the information about concomitant gastrointestinal symptoms at the time of DH diagnosis It is probable that many of these patients never had clinically relevant symptoms of coeliac disease and thus GSRS would rather assess the effect of gluten-free diet on gastrointestinal symptoms instead of the relevance of coeliac disease symptomatology
Opryszczkowate zapalenie skoacutery jest
schorzeniem skoacuternym
bull nozologia DH jest zwodnicza dla wspoacutełczesnej społeczności
zwłaszcza niedermatologicznej
(opryszczkopodobne zapalenie skoacutery)
bull kontinuum autoimmunizacji i (auto)zapalenia
bull kluczowymi w skoacuternej patologii jawią się eTG i neutrofil
(uchwycenie zjawisk skoacuternych jak najbardziej DH-specyficznych)
bull DH to zapewne choroba skoacuterna z towarzyszącą nadwrażliwością na gluten
nieporozumienia
bull dapson na import docelowy
bull okolica łokciowa
bull pośladek jako miejsce wykonania DIFf
bull
foto Zbyszek KaczmarekGazeta Polska
DH patomechanizm
Uważam że należy postrzegać DH jako chorobę skoacuterną z drugorzędnym udziałem patologii jelitowej
Sądzę że w skoacuternej patogenezie tej dermatozy wspoacutełgrają wzajemnie zapętlone zjawiska autoimmunizacji zależne od kluczowego autoantygenu ndash enzymu transglutaminazy naskoacuterkowej (eTG) przemieszczonej być może w wyniku mikrourazoacutew i drapania do skoacutery właściwej w bliskości połączenia skoacuterno-naskoacuterkowego (dermal-epidermal junction DEJ) z wyższych warstw naskoacuterka gdzie ma ona znaczenie fizjologiczne jako bdquoklej biologicznyrdquo (jeden z elementoacutew bdquobariery naskoacuterkowejrdquobdquokoperty rogowejrdquo) oraz (auto)zapalenia zależnego od uczynnionych neutrofiloacutew uwalniających elastazę neutrofiloacutew (NE) trawiącą DEJ z wytworzeniem rozwarstwienia w przestrzeni lamina lucida
DH postępowanie diagnostyczne
Standardem diagnostyki roacuteżnicowej DH powinno być postępowanie troacutejskładnikowe oparte o badanie kliniczne (co i gdzie)(stereotypowym chorym będzie młodzieniec lub młody mężczyzna) bezpośrednie badanie immunofluorescencyjne (DIF)skoacutery klinicznie niezmienionej z otoczenia wykwitoacutew analogicznie do pozostałych autoimmunizacyjnych dermatoz pęcherzowych (ujawnia definiujące to schorzenie złogi IgA w co najmniej 7 wzorach) oraz oznaczenie surowiczych przeciwciał IgA techniką ELISA z jednym substratem do wyboru z zakresu transglutaminaza tkankowa (tTG) eTG nonapeptydy gliadyny (npG) neoepitopy gliadyna-tTG (neo-tTG) Owo postępowanie można uzupełnić o badanie histologiczne H+E wycinka ze skoacutery wykwitowej i badanie haplotypu HLA DQ2DQ8 u chorych z niejednoznacznym obrazem kliniczno-pracownianym
DH postępowanie lecznicze
Standardem terapeutycznym w DH czyli generalnie postępowaniem terapeutycznym z wyboru powinno natomiast być postępowanie dwuskładnikowe czyli powiązanie leczenia farmakologicznego kluczowym dapsonem i dietetycznego dietą bezglutenową w indywidualizowanych kombinacjach W postępowaniu leczniczym trzeba też uwzględnić całość problemoacutew zdrowotnych chorego
ACTA DERMATO-VENEREOLOGICA REVIEWERacuteS COMMENTS TO THE AUTHOR(S) Re Manuscript 114366 Authors Pasternack et al Title Quality of life and gastrointestinal symptoms in long-term g The authors analysed the HRQoL in DH patients on gluten free diet The topic is interesting however the study design is questionable First af all dermatitis herpetiformis is not a cutaneous manifestation of coeliac disease but it is rather a cutaneous disease associated with coeliac disease Furthermore the healthy group is poorly characterized (eg concomitant diseases are not mentioned at all eg Diabetes arterial hypertension) No comparison was performed regarding the age and gender distribution between DH patients and controls As there are differences within the DH patients regarding males and females a very low proportion of men in control group is an important bias as it seems that gender may be relevant cofactor In addition I would rather expect comparison between DH menhealthy men and DH womenhealthy women rather than between DH menDH women as the HRQOL in DH patients has been shown to be similar to controls The authors claimed that having ongoing skin symptoms at the time of the study had no influence on GSRS PGWB or SF-36 scores and the data are not shown In my opinion it is very probable that lack of significance was related to very small number of patients in the group of active skin lesions I would also expect from the authors to provide the information about concomitant gastrointestinal symptoms at the time of DH diagnosis It is probable that many of these patients never had clinically relevant symptoms of coeliac disease and thus GSRS would rather assess the effect of gluten-free diet on gastrointestinal symptoms instead of the relevance of coeliac disease symptomatology
Opryszczkowate zapalenie skoacutery jest
schorzeniem skoacuternym
bull nozologia DH jest zwodnicza dla wspoacutełczesnej społeczności
zwłaszcza niedermatologicznej
(opryszczkopodobne zapalenie skoacutery)
bull kontinuum autoimmunizacji i (auto)zapalenia
bull kluczowymi w skoacuternej patologii jawią się eTG i neutrofil
(uchwycenie zjawisk skoacuternych jak najbardziej DH-specyficznych)
bull DH to zapewne choroba skoacuterna z towarzyszącą nadwrażliwością na gluten
nieporozumienia
bull dapson na import docelowy
bull okolica łokciowa
bull pośladek jako miejsce wykonania DIFf
bull
foto Zbyszek KaczmarekGazeta Polska
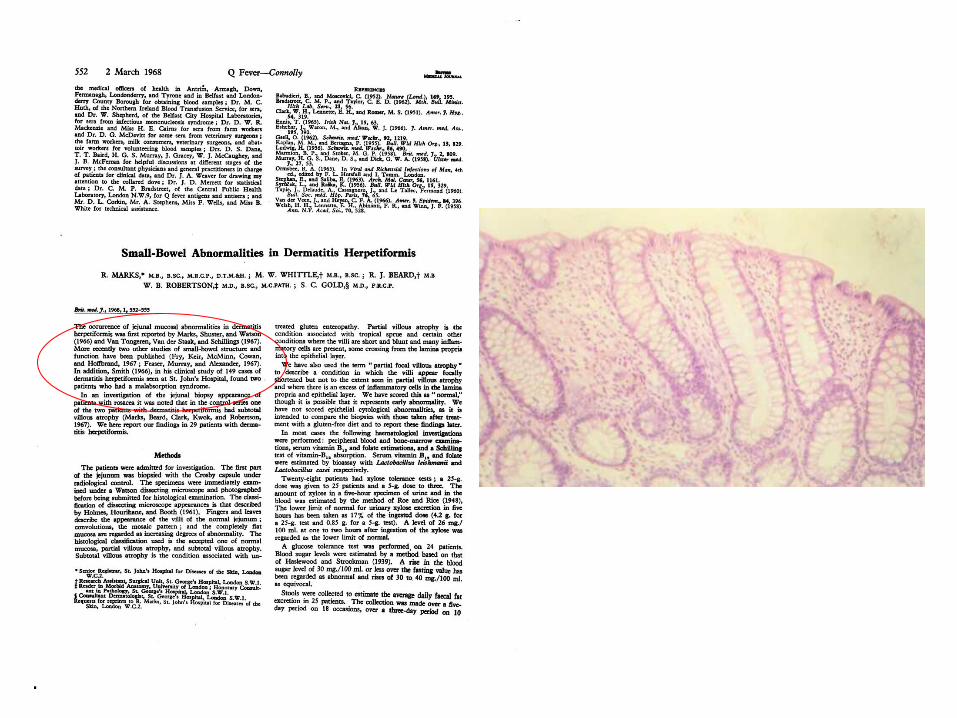
DH postępowanie diagnostyczne
Standardem diagnostyki roacuteżnicowej DH powinno być postępowanie troacutejskładnikowe oparte o badanie kliniczne (co i gdzie)(stereotypowym chorym będzie młodzieniec lub młody mężczyzna) bezpośrednie badanie immunofluorescencyjne (DIF)skoacutery klinicznie niezmienionej z otoczenia wykwitoacutew analogicznie do pozostałych autoimmunizacyjnych dermatoz pęcherzowych (ujawnia definiujące to schorzenie złogi IgA w co najmniej 7 wzorach) oraz oznaczenie surowiczych przeciwciał IgA techniką ELISA z jednym substratem do wyboru z zakresu transglutaminaza tkankowa (tTG) eTG nonapeptydy gliadyny (npG) neoepitopy gliadyna-tTG (neo-tTG) Owo postępowanie można uzupełnić o badanie histologiczne H+E wycinka ze skoacutery wykwitowej i badanie haplotypu HLA DQ2DQ8 u chorych z niejednoznacznym obrazem kliniczno-pracownianym
DH postępowanie lecznicze
Standardem terapeutycznym w DH czyli generalnie postępowaniem terapeutycznym z wyboru powinno natomiast być postępowanie dwuskładnikowe czyli powiązanie leczenia farmakologicznego kluczowym dapsonem i dietetycznego dietą bezglutenową w indywidualizowanych kombinacjach W postępowaniu leczniczym trzeba też uwzględnić całość problemoacutew zdrowotnych chorego
ACTA DERMATO-VENEREOLOGICA REVIEWERacuteS COMMENTS TO THE AUTHOR(S) Re Manuscript 114366 Authors Pasternack et al Title Quality of life and gastrointestinal symptoms in long-term g The authors analysed the HRQoL in DH patients on gluten free diet The topic is interesting however the study design is questionable First af all dermatitis herpetiformis is not a cutaneous manifestation of coeliac disease but it is rather a cutaneous disease associated with coeliac disease Furthermore the healthy group is poorly characterized (eg concomitant diseases are not mentioned at all eg Diabetes arterial hypertension) No comparison was performed regarding the age and gender distribution between DH patients and controls As there are differences within the DH patients regarding males and females a very low proportion of men in control group is an important bias as it seems that gender may be relevant cofactor In addition I would rather expect comparison between DH menhealthy men and DH womenhealthy women rather than between DH menDH women as the HRQOL in DH patients has been shown to be similar to controls The authors claimed that having ongoing skin symptoms at the time of the study had no influence on GSRS PGWB or SF-36 scores and the data are not shown In my opinion it is very probable that lack of significance was related to very small number of patients in the group of active skin lesions I would also expect from the authors to provide the information about concomitant gastrointestinal symptoms at the time of DH diagnosis It is probable that many of these patients never had clinically relevant symptoms of coeliac disease and thus GSRS would rather assess the effect of gluten-free diet on gastrointestinal symptoms instead of the relevance of coeliac disease symptomatology
Opryszczkowate zapalenie skoacutery jest
schorzeniem skoacuternym
bull nozologia DH jest zwodnicza dla wspoacutełczesnej społeczności
zwłaszcza niedermatologicznej
(opryszczkopodobne zapalenie skoacutery)
bull kontinuum autoimmunizacji i (auto)zapalenia
bull kluczowymi w skoacuternej patologii jawią się eTG i neutrofil
(uchwycenie zjawisk skoacuternych jak najbardziej DH-specyficznych)
bull DH to zapewne choroba skoacuterna z towarzyszącą nadwrażliwością na gluten
nieporozumienia
bull dapson na import docelowy
bull okolica łokciowa
bull pośladek jako miejsce wykonania DIFf
bull
foto Zbyszek KaczmarekGazeta Polska

DH postępowanie lecznicze
Standardem terapeutycznym w DH czyli generalnie postępowaniem terapeutycznym z wyboru powinno natomiast być postępowanie dwuskładnikowe czyli powiązanie leczenia farmakologicznego kluczowym dapsonem i dietetycznego dietą bezglutenową w indywidualizowanych kombinacjach W postępowaniu leczniczym trzeba też uwzględnić całość problemoacutew zdrowotnych chorego
ACTA DERMATO-VENEREOLOGICA REVIEWERacuteS COMMENTS TO THE AUTHOR(S) Re Manuscript 114366 Authors Pasternack et al Title Quality of life and gastrointestinal symptoms in long-term g The authors analysed the HRQoL in DH patients on gluten free diet The topic is interesting however the study design is questionable First af all dermatitis herpetiformis is not a cutaneous manifestation of coeliac disease but it is rather a cutaneous disease associated with coeliac disease Furthermore the healthy group is poorly characterized (eg concomitant diseases are not mentioned at all eg Diabetes arterial hypertension) No comparison was performed regarding the age and gender distribution between DH patients and controls As there are differences within the DH patients regarding males and females a very low proportion of men in control group is an important bias as it seems that gender may be relevant cofactor In addition I would rather expect comparison between DH menhealthy men and DH womenhealthy women rather than between DH menDH women as the HRQOL in DH patients has been shown to be similar to controls The authors claimed that having ongoing skin symptoms at the time of the study had no influence on GSRS PGWB or SF-36 scores and the data are not shown In my opinion it is very probable that lack of significance was related to very small number of patients in the group of active skin lesions I would also expect from the authors to provide the information about concomitant gastrointestinal symptoms at the time of DH diagnosis It is probable that many of these patients never had clinically relevant symptoms of coeliac disease and thus GSRS would rather assess the effect of gluten-free diet on gastrointestinal symptoms instead of the relevance of coeliac disease symptomatology
Opryszczkowate zapalenie skoacutery jest
schorzeniem skoacuternym
bull nozologia DH jest zwodnicza dla wspoacutełczesnej społeczności
zwłaszcza niedermatologicznej
(opryszczkopodobne zapalenie skoacutery)
bull kontinuum autoimmunizacji i (auto)zapalenia
bull kluczowymi w skoacuternej patologii jawią się eTG i neutrofil
(uchwycenie zjawisk skoacuternych jak najbardziej DH-specyficznych)
bull DH to zapewne choroba skoacuterna z towarzyszącą nadwrażliwością na gluten
nieporozumienia
bull dapson na import docelowy
bull okolica łokciowa
bull pośladek jako miejsce wykonania DIFf
bull
foto Zbyszek KaczmarekGazeta Polska
ACTA DERMATO-VENEREOLOGICA REVIEWERacuteS COMMENTS TO THE AUTHOR(S) Re Manuscript 114366 Authors Pasternack et al Title Quality of life and gastrointestinal symptoms in long-term g The authors analysed the HRQoL in DH patients on gluten free diet The topic is interesting however the study design is questionable First af all dermatitis herpetiformis is not a cutaneous manifestation of coeliac disease but it is rather a cutaneous disease associated with coeliac disease Furthermore the healthy group is poorly characterized (eg concomitant diseases are not mentioned at all eg Diabetes arterial hypertension) No comparison was performed regarding the age and gender distribution between DH patients and controls As there are differences within the DH patients regarding males and females a very low proportion of men in control group is an important bias as it seems that gender may be relevant cofactor In addition I would rather expect comparison between DH menhealthy men and DH womenhealthy women rather than between DH menDH women as the HRQOL in DH patients has been shown to be similar to controls The authors claimed that having ongoing skin symptoms at the time of the study had no influence on GSRS PGWB or SF-36 scores and the data are not shown In my opinion it is very probable that lack of significance was related to very small number of patients in the group of active skin lesions I would also expect from the authors to provide the information about concomitant gastrointestinal symptoms at the time of DH diagnosis It is probable that many of these patients never had clinically relevant symptoms of coeliac disease and thus GSRS would rather assess the effect of gluten-free diet on gastrointestinal symptoms instead of the relevance of coeliac disease symptomatology
Opryszczkowate zapalenie skoacutery jest
schorzeniem skoacuternym
bull nozologia DH jest zwodnicza dla wspoacutełczesnej społeczności
zwłaszcza niedermatologicznej
(opryszczkopodobne zapalenie skoacutery)
bull kontinuum autoimmunizacji i (auto)zapalenia
bull kluczowymi w skoacuternej patologii jawią się eTG i neutrofil
(uchwycenie zjawisk skoacuternych jak najbardziej DH-specyficznych)
bull DH to zapewne choroba skoacuterna z towarzyszącą nadwrażliwością na gluten
nieporozumienia
bull dapson na import docelowy
bull okolica łokciowa
bull pośladek jako miejsce wykonania DIFf
bull
foto Zbyszek KaczmarekGazeta Polska
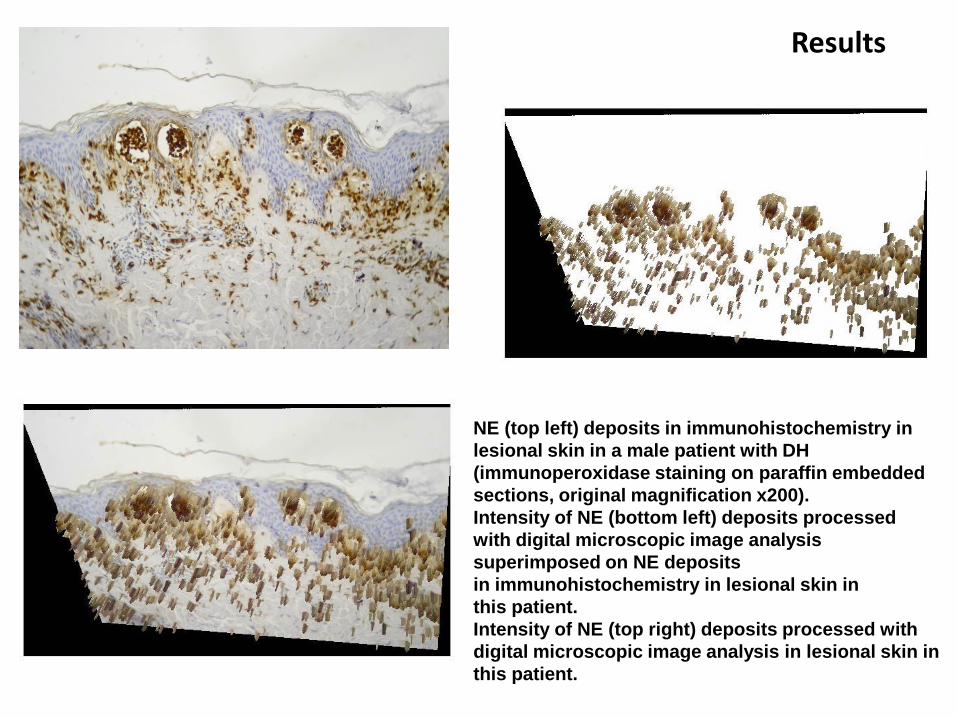
Opryszczkowate zapalenie skoacutery jest
schorzeniem skoacuternym
bull nozologia DH jest zwodnicza dla wspoacutełczesnej społeczności
zwłaszcza niedermatologicznej
(opryszczkopodobne zapalenie skoacutery)
bull kontinuum autoimmunizacji i (auto)zapalenia
bull kluczowymi w skoacuternej patologii jawią się eTG i neutrofil
(uchwycenie zjawisk skoacuternych jak najbardziej DH-specyficznych)
bull DH to zapewne choroba skoacuterna z towarzyszącą nadwrażliwością na gluten
nieporozumienia
bull dapson na import docelowy
bull okolica łokciowa
bull pośladek jako miejsce wykonania DIFf
bull
foto Zbyszek KaczmarekGazeta Polska