Embed Size (px)
Citation preview

Page 1 of 31
CYFARFOD BWRDD IECHYD PRIFYSGOL UNIVERSITY HEALTH BOARD MEETING
DYDDIAD Y CYFARFOD: DATE OF MEETING: 30th March 2017
TEITL YR ADRODDIAD: TITLE OF REPORT:
Integrated Performance Assurance Report Month 11 - 2016/17
CYFARWYDDWR ARWEINIOL: LEAD DIRECTOR:
Karen Miles, Director of Planning, Performance & Commissioning In association with all Executive Leads
SWYDDOG ADRODD: REPORTING OFFICER:
Karen Miles, Director of Planning, Performance & Commissioning
Pwrpas yr Adroddiad (dilewch fel yn addas) Purpose of the Report (delete as appropriate)
Ar Gyfer Penderfyniad For Decision
Ar Gyfer Trafodaeth For Discussion
Er Gwybodaeth For Information
√
ADRODDIAD SCAA SBAR REPORT Sefyllfa / Situation A revised Welsh Health Circular (2016) 023 on the ‘NHS Outcome Framework and Measures Guidance 2016/17’ was issued by Welsh Government on 29th March 2016. The outcome indicators (referenced as ‘measures’) included in the Framework aim to provide an annual view of the impact health services are having on improving outcomes at a population level, and each indicator has a Welsh Government target which Health Boards need to achieve. As was the case in 2015/16, the Framework incorporates seven domains which specify what people can expect from the National Health Service (NHS) in Wales as follows:
• Staying healthy – I am well informed and supported to manage my own physical and mental health
• Safe care – I am protected from harm and protect myself from known harm • Effective care – I receive the right care and support as locally as possible and I contribute to
making that care successful • Dignified care – I am treated with dignity and respect and treat others the same • Timely care – I have access to services based on clinical need and am actively involved in
decisions about my care • Individual care – I am treated as an individual, with my own needs and responsibilities • Our staff and resources – I can find information about how the NHS is open and transparent
on its use of resources and I can make careful use of them Cefndir / Background Our aim is to develop a fully integrated performance report that provides assurance to Hywel Dda University Health Board (HDUHB), on the most recent outturn position, for key deliverable areas. In addition to this, a hyperlink is also provided to the last fully detailed Integrated Performance report, Month 10 2016/17. Performance has been RAG - rated (red; amber; green), as per the following ‘key’, and in line with Board member requests on the same and throughout the report, we have included our All Wales ranking and wherever possible, number counts as well as percentages. Also some other

Page 2 of 31
associated terms have been further explained.
Target not delivered
Within 5% of target* Target delivered
Est. – Estimated N/A – not available R12 rolling – rolling 12 month period
* For measures where there is a reduction or improvement target, these will only be scored red or green. This also applies to measures with a small percentage target (10% and under), e.g. Sickness/absence, smoking cessation. For measures where the target is 0, these will only be scored red or green. Green for 0, red for anything above.
Asesiad / Assessment Key Deliverable Areas The table below demonstrates the 22 key deliverable measures. 12 are currently successful or in close proximity of being successful, and the remaining 10 are classed as non successful. This position represents a slight improvement compared to month 10 by 1 measure. Using the latest All Wales published data; the Health Board is performing first in 7 of these measures and is in the top three of the remaining 15 measures.

Page 3 of 31
Within the report, certain key deliverable measures which bring together the ‘pathway’ challenges have been grouped by Directorate, irrespective of the Domain they sit within. A set of 4 dashboards, Unscheduled Care; Scheduled Care; Hospital Acquired Infections (under development); Oncology & Cancer have been included in an attempt to contextualise the Directorates’ overall performance and run in the following order:
• The first part of each Dashboard notes current performance for key metrics • The second part provides a view of current finances and workforce measures
using the latest available outturn • The third part of the dashboard contextualises Hywel Dda University Health Board (HDUHB)
performance against All Wales, using latest available outturn • In time, we would want a fourth part to properly capture patient outcomes and experience
The Domain name shown in brackets at the beginning of each section denotes where the previous month 10 brief can be found in the full performance report, available via the following link: http://www.wales.nhs.uk/sitesplus/documents/862/Item08i.IntegratedPerformanceAssuranceReport.pdf

Page 4 of 31
Unscheduled Care (see Integrated Performance Assurance Report: hyperlink on page 3 - Timely Care Domain)
Note: proxy vacancy figures reflect the difference between the budgeted establishment in Whole Time Equivalents (WTE) compared to actual (WTE) staff in post.
Delayed Transfer of Care (Local
Authority Area)
Red Calls (estimate)
>1 hour Handovers <4 hour wait >12 hour wait
Direct to Stroke Unit <4 hours
CT <12 hours
Assessed by Stroke
Consultant < 24 hours
Thrombolysed patients door to needle <=
45mins
Non mental health
(aged 75+) per 10,000
LHB population
64.3% 91 84.2% 382 70.2% 100.0% 73.7% 44.4% 59.7
Budget to date 109.039 Premium Pay 12.626 1% CIP Target 0.984 Spend to date 122.140 Variable Pay 25.585 Delivery 0.468 Variance overspe 13.101 Variance 0.516% Variance 12.0% % Variance 52.4%
Delayed Transfer of
Care
Red Calls >1 hour Handovers <4 hour wait >12 hour wait
Direct to Stroke Unit <4 hours
CT <12 hours
Assessed by Stroke
Consultant < 24 hours
Thrombolysed patients door to needle <=
45mins
Non mental health
(aged 75+) per 10,000
LHB population
76.1% 178 82.8% 547 70.5% 100.0% 80.4% 27.3% 61.3
3rd out of 7 2nd out of 6 1st out of 6 3rd out of 6 1st out of 6 Joint 1st out of 6 2nd out of 6 3rd out of 6 1st out of 7
75.4% 2,972 79.0% 4,069 44.4% 94.7% 75.9% 25.5% 157.9
Proxy vacancies (budget vs actual wte) (Month 11) including Pathology & RadiologySickness (R12m end January 2017)
Finance (Year to Date - Month 11) - including Pathology & Radiology
5.34%
Unscheduled Care Dashboard - February 2017
Staffing
Ambulance A&E Waits Stroke
48.72
Lead Executive - Joe Teape Responsible Officers - Sarah Perry, Hazel Davies, Brett Denning, John Evans
All Wales Performance
Last available All Wales data published February 2017Ranking (1st being the best and 7th being the worst)
Hywel Dda Performance & Position in Wales
StrokeA&E WaitsAmbulance
Budget (£m) Pay (£m) Agency Fees (£m)
0.870
1% CIP Target (£m)

Page 5 of 31
Ambulance Red Calls
Provisional February 2017 data showed Red performance closed at 64.3% (January 2017, 76.1%), a 12% decline, which reversed the progress over the previous months. If a further 3 Red calls had been responded to within the 8 minutes, the target would have been met. The table below shows the month on month breakdown by County and call type: Red Calls February 2017 January 2017 Carmarthenshire 66.1% 77.5 Ceredigion 64.0% 69.0% Pembrokeshire 61.3% 78.1% Amber Calls Carmarthenshire 58.4% 59.1% Ceredigion 71.6% 65.7% Pembrokeshire 71.0% 72.7% Amber Calls Amber 1-20 minute target 1,636 1,799 Amber 2-30 minute target 875 994
The conveyance rate is 72.2% which is 12.2% above the 60% target. 9.8% of patients were treated at the scene which is 10.2% less than the 20% target. In February, the Welsh Ambulance Service NHS Trust (WAST) reduced the Resource Escalation Action Plan (REAP) level to 1, which in theory allowed normal operational activity to resume across Wales. This did result in increased cross border activity, with Hywel Dda vehicles being deployed and retained in Abertawe Bro Morgannwg University Health Board (ABMUHB) if they were the closest available resource. During mid-February it was agreed that both Hywel Dda and Powys would resume REAP 3 actions to support performance, all response capable managers were placed in to the performance plan to support operations.

Page 6 of 31
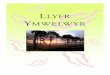
Ambulance Handovers and A&E 4 and 12 Hour Performance As a Health Board, overall Unscheduled Care has seen a performance improvement when comparing February 2017 to January 2017, which was a significantly challenging month across the board. The number of Ambulance handovers over 1 hour, is not comparable on a month on month basis, due to the reduced number of days in February. However, based on average daily numbers, performance has improved:
• The number of ambulance handovers over 1 hour improved from a January daily average of 5.7 to 3.3 in February.
• Patients waiting in A&E less than 4 hours improved from 82.8% in January to 84.2% in February.
• Performance has improved for the number of patients seen in A&E within 12 hours, from 95.1% in January to 96.4% in February.
Despite an overall rise of circa 5% in the year to date attendances, January 4 hour waiting times outturn of 82.8% was the best in Wales. Similarly, with the rate of Non Mental Health Delayed Transfers of Care reducing in January 2017, the Health Board was ranked the best in Wales.
February 2017 Ambulance Arrivals
New Attendances
4 HourNational Target
4 Hour Performance
4 Hour Breaches
12 HourNational Target
12 Hour Performance
12 Hour Breaches
Bronglais General Hospital 438 2,057 95% 88.19% 243 0 98.98% 21Glangwili General Hospital 1,025 3,049 95% 80.42% 597 0 93.74% 191Prince Philip Hospital (MIU Only) 475 2,231 95% 96.68% 74 0 99.91% 2Withybush General Hospital 804 2,979 95% 75.06% 743 0 94.36% 168Health Board * 2,742 10,472 95% 84.18% 1,657 0 96.35% 382* The figures for the Health Board include Llandovery and Cardigan Minor Injury units
0
20
40
60
80
100
120
140
160
180
Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17
No. o
f Han
dove
rs
Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17BGH 16 11 8 21 16 23 16 3 8 32 15GGH 79 67 38 48 54 33 35 35 48 93 43PPH 13 1 0 6 3 0 3 3 1 30 23WGH 6 9 11 1 2 21 4 28 26 23 10HDUHB 114 88 57 76 75 77 58 69 83 178 91HDUHB Trajectory 154 132 85 50 40 27 22 22 17 25 23
Hywel Dda University Health Board - Ambulance Handovers over 1 hour, Target = 0

Page 7 of 31
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17
% P
erfo
rman
ce
Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17BGH 87.52% 89.10% 89.59% 90.68% 91.49% 90.40% 87.50% 93.74% 88.83% 87.08% 88.19%GGH 78.74% 77.47% 82.02% 82.72% 80.07% 74.07% 80.86% 80.35% 80.17% 76.25% 80.42%PPH 95.92% 98.21% 96.17% 96.52% 97.84% 97.88% 96.59% 96.87% 98.11% 95.84% 96.68%WGH 72.49% 74.94% 72.12% 83.86% 81.08% 74.95% 78.34% 77.39% 74.11% 75.84% 75.06%HDUHB 83.09% 83.94% 84.15% 87.86% 86.56% 83.02% 85.15% 86.19% 84.18% 82.79% 84.18%HDUHB Trajectory 83.0% 85.0% 86.0% 86.0% 86.0% 87.0% 89.0% 89.0% 87.0% 84.0% 85.0%
Hywel Dda University Health Board - 4 hour A & E Performance, Target = 95%
0%5%
10%15%20%25%30%35%40%45%50%55%60%65%70%75%80%85%90%95%
100%
Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17
% P
erfo
rman
ce
Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17BGH 99.00% 99.13% 99.25% 99.30% 99.10% 99.22% 97.96% 99.14% 98.69% 97.42% 98.98%GGH 94.57% 96.14% 95.16% 95.16% 95.15% 93.45% 94.75% 94.16% 93.51% 90.75% 93.74%PPH 99.30% 99.89% 99.89% 99.93% 99.96% 100.00% 99.92% 100.00% 99.96% 99.38% 99.91%WGH 93.47% 95.63% 94.90% 98.65% 97.92% 95.44% 96.51% 94.01% 94.95% 94.68% 94.36%HDUHB 96.31% 97.47% 96.99% 98.06% 97.80% 96.66% 97.08% 96.49% 96.36% 95.11% 96.35%
Hywel Dda University Health Board - 12 hour A & E Performance

Page 8 of 31
Whilst the HDUHB over arching improved performance is summarised above, the individual acute site performance variances are outlined in further detail below, giving a flavour of their challenges. Bronglais General Hospital (BGH)
• In general, February has seen an improvement in terms of site pressures and performance compared to January 2017, which was a significantly challenging month across the board:
o Ambulance handovers over 1 hour improved from a January daily average of 1, to 0.5 in February
o 4 hour performance has increased by 1.11% to 88.19% compared to the previous month, with the top breach reason remaining as access to Medical beds
o Performance has improved for the number of patients waiting in A&E 12 hours or more, with 98.98% of patients seen within 12 hours in February compared to 97.42% in January
• February has seen a significant improvement in ambulance handover delays, there is
detailed daily focus by the team and this should continue. A further breakdown of handover performance indicates that 15 minute handover has improved but 1 hour delays, though small in number, require focus. This again is linked to majors and admitted performance due to the need for better discharge planning to create ward capacity.
• There has been a slight 1% improvement in 4 hour A & E performance, compared to last
month. The majority of attendees are minors and yet the non admitted performance is meeting the 95% trajectory. The focus therefore needs to be on admitted performance and to achieve that there will be considerable focus on working with ward teams (medical and nursing) to improve the discharge process to create capacity, and therefore improve admitted performance.
• An agreement has been reached to establish what will be entitled “The Bronglais Clinical Forum”; the membership of this group will include Medics and Nurses working with the operational team. Terms of Reference state the group will meet formally each month with the aim of delivering the necessary improvements and monitoring progress etc. Work streams falling out of this are also established to focus on more localised needs.
Glangwili General Hospital (GGH) • Performance has improved in February:
o Ambulance handovers over 1 hour improved from a January daily average of 3 to 1.5 in February
o 4 hour performance has increased by 4.17% to 80.42% compared to the previous month, with the top breach reason remaining as access to Medical beds
o Performance has improved for the number of patients waiting in A&E 12 hours or more, with 93.74% of patients seen within 12 hours in February, compared to 90.75% in January
• Overnight patients in A&E requiring inpatient beds continues to cause 4 hour breaches, the
department is then full and has difficulty in assessing and treating new patients. The use of the Clinical Decisions Unit (CDU) as an overnight bedded area, decreased in February 2017 whilst maintaining half of ambulatory care, to allow some of the GP expected patients to be seen in CDU.
• The hospital continues to see an increase in the acuity and complexity of patients requiring Medical care and supported discharge. Nurse staffing on the wards remains a concern, and reliance on bank and agency staff. There is continued recruitment to vacancies but with known staff leaving, there will be no net increase over the next 2 months.

Page 9 of 31
• Red and green days have been implemented on all of the Medical wards in February 2017
and will now extend to include the stroke and cardiac wards. A database has been developed to identify the number of patients who have red days, the reason why and actions to address why the patient is experiencing a delay.
• The CDU model is being developed with the consultants and the revised operational policy will be in place by the end of March 2017. This will see improved use of the ambulatory care area and clinics to enable timely patient review and follow up.
• The discharge lounge has an average throughput of 50 patients per week. The discharge lounge sister is reviewing the area to expand the capacity of the number of stretcher discharges that can be accommodated. The focus is now on increasing use before 10am to enable flow through A&E and CDU.
Prince Philip Hospital (PPH) • PPH maintained good 4 hour performance during February and delivered an improvement
across all of the key Unscheduled Care performance areas compared to January 2017: o Ambulance handovers over 1 hour improved from a January daily average of 0.9
to 0.8 in February o 4 hour performance increased by 0.84% to 96.68%, with the top breach reason
remaining as access to A & E clinicians o Performance has improved for the number of patients waiting in A&E 12 hours or
more, with 99.91% of patients seen within 12 hours in February, compared to 99.38% in January
• Ambulance offload delays were the main challenge for the site in February, with 23 patients
waiting over 1 hour to be offloaded. 12 of the offload delays occurred on one day in early February, where there were multiple ward closures due to infection outbreaks.
• The PPH team, in conjunction with Carmarthenshire community, continue to make improvements to the Unscheduled Care system as part of the rolling improvement plans, and this includes the development of alternative areas to surge beds at times of extreme pressure.
Withybush General Hospital (WGH)
• February Performance: o Ambulance handovers over 1 hour improved from a January daily average of 0.7
to 0.4 in February o 4 hour performance decreased by 0.78% to 75.06% compared to the previous
month, with the top breach reason remaining as access to Medical beds o Performance has decreased slightly for the number of patients waiting in A&E 12
hours or more, with 94.36% of patients seen within 12 hours in February compared to 94.68% in January
• Additional activity was experienced within the A&E department compared to the same month
of the previous year. This rise and a greater proportional split of Major’s to Minor’s in the last 12 months, can be attributed to the amendment of the ambulance divert borders from 1st September 2016 of circa 5 admissions per day.
• The main challenge for February has been the flow of patients between the A&E department and Medical Wards. An increase in demand and a shortage of beds have led to increased

Page 10 of 31
numbers of unplaced medical patients, both in Major and Minor spaces within the department. The minor’s stream has therefore proved difficult to maintain, due to the occupation of majors within the see and treat rooms.
• A 4 week audit by the Hospital Service Manager of all A&E process and breach reasons has been put in place, commencing March 1st. The results of which will inform the site team, to enable change, improve efficiencies and to differentiate between what are bed capacity issues and what are system failings. This review has been fully communicated and accepted by the department.
Stroke Stroke admissions remain comparable to the month before with 57 Stroke admissions in February 2017. Admissions comprised of 6 from Bronglais General Hospital (BGH), 25 from Glangwili General Hospital (GGH), 10 from Prince Philip Hospital (PPH) and 16 from Withybush General Hospital (WGH).
• Admissions to the Stroke unit within 4 hours has shown an upwards trend since June 2016. This
trend continues with 70.2% of patients meeting the target in February 2017. • Hywel Dda University Health Board (HDUHB) continues to perform well with regards to scanning
patients within 12 hours, remaining at 100% for the fourth consecutive month. • The Health Board position for being assessed by a Stroke Consultant within 24 hours is currently
73.7%, which is a decrease compared to last month (80.4%) but an improvement on 55.4% reported in December 2016.
• Thrombolysed patients with Door-to-Needle <= 45 minutes performance has shown an improvement for the second month running, from 27.3% in January to 44.4% in February 2017.
• The most recent All Wales performance data, published in February 2017 shows the latest Health Board position as follows:
o 1st in Wales for Direct admission to a Stroke Unit within 4 hours o Joint 1st in Wales for CT scan within 12 hours o 2nd in Wales for being assessed by a Stroke Consultant <24 hours

Page 11 of 31
o 3rd in Wales for Thrombolysing patients with door-to-needle <= 45 minutes There has been a shift in 4 hour performance across individual sites in February. Prince Philip, Glangwili and Bronglais hospitals have seen an improvement in admitting patients to the Acute Stroke Unit (ASU) within 4 hours, however Withybush has seen a significant drop in performance in this measure. Analysis of Withybush Hospital’s performance indicates communication issues between A&E and the Stroke teams, resulting in a delay in initiating the Stroke pathway on some occasions. To address this, the Stroke Specialist Nurses have planned weekly Stroke education sessions in A&E and are raising issues regarding inconsistent attendance at the weekly Stroke Improvement meetings. 72 Hour Pathway Care:

Page 12 of 31
Thrombolysis Care:
Financial Update The Unscheduled Care Directorate is £13.101m overspent, of which premium variable pay above funded establishment is £12.626m. Gross variable pay is £25.585m and the point to note is that whilst vacancies contribute/offset these costs, the cost of inefficiency/poor productivity because of teams working in an ad hoc way, either because staff are external or because of overtime has an impact on all indicators. Sickness rates have further deteriorated from 5.1% to 5.34% this month, thus remaining above the 4.79% target and there are an approximate 49 WTE vacancies. About 48% of the Cost Improvement Plan (CIP) savings to date have been delivered, although £0.225m of the target remains unidentified.

Page 13 of 31
Scheduled Care (see Integrated Performance Assurance Report: hyperlink on page 3- Timely Care Domain)
Note: proxy vacancy figures reflect the difference between the budgeted establishment in Whole Time Equivalents (WTE) compared to actual (WTE) staff in post.
Total open pathways
Total >36 weeks
Total open pathways
Total < 26 weeks
54,922 4,059 54,922 46,043
Budget to date 101.121 Premium Pay 6.371 1% CIP Target 0.792Spend to date 110.081 Variable Pay 12.373 Delivery 0.48Variance overspend 8.960 Variance 0.312% Variance 8.9% % Variance 39%
0 40% (Jan 2017)
25,089
Staffing
7.4%
Sickness (R12m end January 2017) Proxy vacancies (budget vs actual wte) (Month 11)
101.655.16%
83.8%
Finance (Year to Date - Month 11)
Delayed Follow UpsReferral To Treatment
Ranking (1st being the best and 7th being the worst)Last available All Wales data published February 2017
Diagnostic Waits Postponed Procedures
Scheduled Care Dashboard - February 2017
Treated <14 days
Postponed Procedures
Waits >36 wks (Feb-17)
Responsible Officer - Stephanie Hire
Waits <26 Wks (Feb-17) Waits >8 weeks
Diagnostic Waits Delayed Follow Ups
Wait >Target Date
Referral To Treatment
Lead Executive - Joe Teape
301,72540.9%9,41485.7%21,387
Waits >36 wks Waits <26 Wks Waits > 8 weeks
6th out of 7
4,827
7th out of 7
81.4%
Hywel Dda Performance & Position in Wales
Treated <14 days Wait >Target Date
1st out of 6th
76.9% 29,318
3rd out of 7
0
1st out of 7
Budget (£m)
0.736
Pay (£m) Agency Fees (£m) 1% CIP Target (£m)

Page 14 of 31
Referral to Treatment Time The percentage of patients treated within 26 weeks has improved from 81.4% in January to 83.8% at the end of February 2017; representing the highest performance during this financial year.
36 week breach numbers have reduced from 4,827 last month to 4,059; representing the lowest breach numbers reported during this financial year. Patients waiting 52 weeks or more have decreased from 1,327 in January to 1,167 at the end of February 2017. Update on the end of financial year position
• The Health Board’s continuing aim is to reduce 36 week breach numbers to below 4,000 by the end of March 2017.
• A communications plan and letter is being developed to send to all breach cohort patients at the end of March 2017, with an anticipated plan of treatment times. This is being developed in collaboration with the Community Health Council (CHC).

Page 15 of 31
Diagnostic Waits over 8 weeks In February 2017, the Health Board maintained a zero breach position for the fifth month running. Each area maintained their position by following their current plans, outlined as follows:
• Radiology are using overtime and bank working. • Cardiology Heads of Service continually monitor diagnostic lists closely. The department is
supported by locum echo-cardiographers that are in the process of being recruited on a substantive basis.
• In Urodynamics, the department is continuing to offer respective tests at different sites until staffing levels are replaced.
• In Endoscopy, Service Managers and waiting list teams continually monitor patient lists to resolve potential breaches.
Postponed Admitted Procedures (Programme for Government Commitment) At the end of January 2017, postponed procedures treated in less than 14 days have met the 12 month improvement target. 45 procedures were postponed on more than 1 occasion, for non clinical reasons. The majority of patients cancelled were Orthopaedic patients at Prince Philip Hospital (PPH). This was due to increased emergency demand and a lack of available beds. However, 40% (18 patients) were treated within the 14 day Programme for Government Commitment. The majority of patients have been rescheduled, with the exception of 10 patients.
Unscheduled care pressures in January 2017, led to a higher than expected number of Postponed Admitted Procedures during the month. Across each site, there was a general increase in the acuity and complexity of unscheduled care patients requiring acute medical care, with the split of Major versus Minor A & E attendances increasing by 3.7% compared to the prior month. For example in January 2017, PPH emergency admissions increased to 777, representing an increase of 253 more

Page 16 of 31
than in January 2016, thus impacting upon flow and elective cases being cancelled. Prince Phillip had emergency admissions that significantly exceeded the numbers expected e.g. on Friday 6th January 2017, the predicted admissions for the day were 23 but by the end of the day 40 patients had been admitted. Delayed Follow Up Appointments Patients waiting for a follow-up appointment past their target date have reduced down to 25,089, resulting in the 12 month reduction target being met. Notable reductions, circa 700, have been witnessed in Surgery and Ophthalmology.
A significant validation exercise has been carried out by an external company, which has resulted in a reduced volume of follow - ups, both booked with no delay and booked with a delay. The Health Board plans to continue this process on the outstanding volume of patients not booked beyond a target date, by working collaboratively with Primary and Acute care colleagues, to clinically validate and review the patients as required. Financial Update The Scheduled Care Directorate is £8.960m overspent, of which premium variable pay above funded establishment is £6.371m. Gross variable pay is £12.373m, and the issues outlined for high levels of non-core staffing in Unscheduled Care are also applicable here. Sickness rates have increased slightly from 5.1% to 5.16% this month and remain above the 4.79% target. There are an approximate 102 WTE vacancies. At month 11, the Directorate has achieved 61% of its year to date Cost Improvement Plan (CIP).

Page 17 of 31
Healthcare Acquired Infections (HCAI’s) (see Integrated Performance Assurance Report: hyperlink on page 3 – Safe Care Domain)
C. difficile During February 2017, the C.difficile target of ensuring a rate of no more than 28/100,000 per population has not been met and is reported as 40.37. Our current ranking against other Health Boards in Wales is 5th from 6. The table below shows the cumulative monthly numbers of C.difficile to achieve the 6 month (Oct 2016 to Mar 2017) reduction expectation and current cumulative monthly numbers for Oct 2016 to Feb 2017.
Mar-17 53 NLAFeb-17 44 64 20 NLA 40.37Jan-17 35 58 23 NLA 44.91Dec-16 26 43 17 43 44.52Nov-16 17 26 9 26 40.60Oct-16 8 9 1 9 27.65
Mth-Yr Maximum cumulative monthly numbers of C. difficile to achieve
reduction expectation
Current cumulative monthly numbers
of C. difficile
Difference between current and expected cumulative monthly
numbers of C. difficile
Revised maximum cumulative monthly
numbers of C. difficile to achieve
reduction expectation
Current cumulative monthly rate of
C. difficile /100,000 population

Page 18 of 31
During February 2017, a review of November/December C.difficile cases in Prince Phillip Hospital was carried out using Start Smart Then Focus Antimicrobial criteria with the following actions to be taken forward:
• Learning to be fed back to the Medical Director for dissemination to Medical Teams. • Root Cause Analysis Proforma is to be adjusted to include Start Smart Then Focus
Antimicrobial prescribing criteria. S. aureus bacteraemia infections During February 2017, the target for S.aureus bacteraemia of ensuring a rate of no more than 20/100,000 per population has not been met and is reported as 34.06. Our current ranking against other Health Boards in Wales is 3rd out of 6. The table below shows the cumulative monthly numbers of S. aureus bacteraemia to achieve the 6 month (Oct 2016 to Mar 2017) reduction expectation and current cumulative monthly numbers for Oct 2016 to Feb 2017.
The following actions are to be taken forward to reduce S. aureus Blood Culture figures:
• Training on Obtaining Blood Cultures carried out in Bronglais Hospital. • Above training to be arranged for Glangwili, Prince Philip and Withybush Hospitals. • Working with the Resuscitation Team on introducing and evaluating the benefits of Sepsis
Boxes to include Cannula and Blood Culture packs, ensuring the use of packs in an emergency situation.
• STOP campaign i.e. prevalence survey of Peripheral Venous Cannulas & Urinary Catheters to be carried out in March. This will give an indication of the appropriateness of devices usage.
Respiratory Cases:
• 2 of the 14 S. aureus cases were respiratory. • Since the beginning of 2017 the Health Board has 112 positive Flu A cases and 1 Flu B case
in hospital (40 cases in the same timeframe in 2016). Delayed Transfers of Care (Mental Health DTOC) (see Integrated Performance Assurance Report: hyperlink on page 3 – Effective Care) As at the end of February 2017, the reduction (12 month trend) target has been met. The latest All Wales data published in February 2017, ranked Hywel Dda University Health Board
Mar-17 38 NLAFeb-17 31 54 23 NLA 34.06Jan-17 25 40 15 NLA 30.97Dec-16 19 32 13 32 33.13Nov-16 12 21 9 21 32.79Oct-16 6 10 4 10 30.72
Mth-Yr Maximum cumulative monthly numbers of
S. aureus bacteraemia to achieve reduction
expectation
Current cumulative monthly numbers
of S. aureus bacteraemia
Difference between current and expected cumulative monthly numbers of S. aureus
bacteraemia
Revised maximum cumulative monthly numbers of S. aureus
bacteraemia to achieve reduction
expectation
Current cumulative monthly rate of
S. aureus bacteraemia
/100,000 population

Page 19 of 31
(HDUHB) 5th out of 7, with a DTOC rate of 4.1. The All Wales performance was 3.7. The table below details the Local Authority (LA) split, year on year:
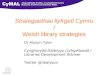
The position in terms of older adult Mental Health DTOCs has fluctuated over the year, but there has been a recent increase in DTOCs in Carmarthenshire. More recently, a number of applications have not been agreed by the County Continuing Heath Care (CHC) process and all of these are being explored to understand how to progress. Delayed Transfers of Care (Non Mental Health DTOC) As at the end of February 2017, the reduction (12 month trend) target has been met. The latest All Wales data published in February 2017, ranked Hywel Dda 1st out of 7 with a DTOC rate of 61.3. This is significantly better than the All Wales performance of 157.9. The table below details the Local Authority (LA) split, year on year.
Performance (February 2017)
Performance (February 2016)
Performance (February 2017)
Performance (February 2016)
Carmarthenshire Local Authority 6.4 3.5 8 10
Ceredigion Local Authority 2.4 3.1 2 3
Pembrokeshire Local Authority 1.5 4.9 6 4
Health Board 4.0 3.9 16 17
Delayed Transfers of Care –Mental Health (Reduction target) - year on year
Delivery per 10,000 population (all ages) - year on year Number of DTOCs - monthly
10 9 7 9 8 16 16 13 14 16 13 17 25 15 8 12 15 10 10 8 7 14 15 16
3.8 3.8 3.7 3.7 3.6 3.8 3.8 3.8 3.8 3.9 3.9 3.94.2
4.4 4.4 4.54.7 4.5 4.4 4.2 4.1 4.0 4.1 4.0
3.8 3.7 3.6 3.5 3.53.3 3.2 3.2 3.2 3.2 3.2
0
1
2
3
4
5
6
0
5
10
15
20
25
Mar
-15
Apr
-15
May
-15
Jun-
15
Jul-1
5
Aug
-15
Sep
-15
Oct
-15
Nov
-15
Dec
-15
Jan-
16
Feb-
16
Mar
-16
Apr
-16
May
-16
Jun-
16
Jul-1
6
Aug
-16
Sep
-16
Oct
-16
Nov
-16
Dec
-16
Jan-
17
Feb-
17
Num
ber p
er10
,000
popu
latio
n
Num
ber
of P
atie
nts
Hywel Dda University Healthboard - Mental Health
Mental Health DTOCs (Local authority) Rolling 12 month DTOC delivery per 10,000 population (all ages) 2016/17 Operational Plan Profile

Page 20 of 31
Performance (February 2017)
Performance (February 2016)
Performance (February 2017)
Performance (February 2016)
Carmarthenshire Local Authority 57.1 72.2 7 17
Ceredigion Local Authority 103.0 74.3 3 3
Pembrokeshire Local Authority 38.4 30.9 3 1
Health Board 59.7 58.7 13 21
Delayed Transfers of Care (DTOC) – Non Mental Health (Reduction target) - year on year
Delivery per 10,000 population (Age 75+) - year on year Number of DTOC's - monthly
16 13 10 23 22 11 19 14 25 22 36 21 35 16 18 24 25 15 23 17 17 15 18 13
64.361.0
57.756.959.257.7
54.9
49.951.953.7
56.958.7
63.564.366.366.667.368.369.370.1
68.166.361.8
59.7
58.758.558.558.558.058.057.557.557.557.557.0
0
10
20
30
40
50
60
70
80
0
5
10
15
20
25
30
35
40
Mar
-15
Apr-1
5
May
-15
Jun-
15
Jul-1
5
Aug-
15
Sep-
15
Oct-1
5
Nov-
15
Dec-
15
Jan-
16
Feb-
16
Mar
-16
Apr-1
6
May
-16
Jun-
16
Jul-1
6
Aug-
16
Sep-
16
Oct-1
6
Nov-
16
Dec-
16
Jan-
17
Feb-
17
Num
ber p
er 10
,000
po
pula
tion
Num
ber
of P
atie
nts
Hywel Dda University Health Board - Non Mental Health
Non Mental Health DTOCs (Local Authority) Rolling 12 month DTOC delivery per 10,000 population (age 75+)
2016/17 Operational Plan Profile

Page 21 of 31
Oncology and Cancer Services (see Integrated Performance Assurance Report: hyperlink page 3 – Timely Care Domain)
Note: proxy vacancy figures reflect the difference between the budgeted establishment in Whole Time Equivalents (WTE) compared to actual (WTE) staff in post. Cancer Waiting Times - Urgent Suspected Cancer (USC) Confirmed performance for January 2017 was 90.9%. Estimated performance for February 2017 is currently 92.8%. The underlying trend in performance improvement during 2016/17 to date is expected to lead to year end performance close to, or in line with profile.
Budget to date 8.319 Premium Pay -0.380 1% CIP Target 0.063 Spend to date 8.317 Variable Pay 0.263 Delivery 0.063 Variance Oversp -0.002 Variance 0.000 % Variance 0.0% % Variance 0.0%
97.1%86.0%
1st in Wales
92.1%
Hywel Dda Performance & Position in Wales
All Wales Performance
3rd in Wales
0.92
1% CIP Target (£m)
Non Urgent Suspected Cancer
Last available All Wales data published February 2017Ranking (1st being the best and 7th being the worst)
Urgent Suspected Cancer
Budget (£m) Pay (£m) Agency Fees (£m)
0.000
98.3%
Oncology & Cancer Services Dashboard - February 2017
Responsible Officer - Keith Jones
Cancer Waiting Times
Urgent Suspected Cancer
Lead Executive - Joe Teape
Estimated 92.8% Estimated 97.6%
Staffing
Non Urgent Suspected Cancer
Sickness (R12m end January 2017) Proxy vacancies (budget vs actual wte) (Month 11)4.90%
Finance (Year to Date - Month 11)

Page 22 of 31
The confirmed performance for January 2017 continues the All Wales performance trend, showing HDUHB ranked 1st amongst the 6 Health Boards in Wales. January performance was based on 9 breaches for the following reasons/areas:
• 2 x complex diagnostic pathways (Head & Neck and UGI pathways) • 2 x tertiary surgery delays (Lung & Urology pathways) • 2 x tertiary oncology delays (Lung & ‘Other’ pathways) • 1 x tertiary diagnostic delay (Gynaecology pathway) • 2 x whole pathway delays (LGI & Skin pathways)
A sustained reduction in the number of patients in the 63 + and 53 to 62 day USC backlog is essential if the Health Board’s performance is to improve in line with agreed profiles. The number of patients in the 63 day and over cohort (currently 18) has reduced since Autumn 2016 and is currently running at its lowest level year to date. There has been significant reduction in the number of patients in the 53 to 62 day cohort (currently 12) since mid September 2016. As with the 62 Day cohort, this cohort is currently running at its lowest range year to date. Cancer Waiting Times – Non Urgent Suspected Cancer (NUSC) Performance year to date has generally exceeded or been within 1% of target (with the exception of November when HDUHB performance was significantly compromised due to treatment delays at the tertiary centre). Confirmed performance for January 2017 was 98.04% (on target and profile). The underlying trend in performance improvement during 2016/17 to date is expected to lead to year end performance close to or in line with profile. The latest All Wales published data shows HDUHB ranked 3rd however a more recent internal performance position of 99.1% will improve the ranking to be 1st in Wales.

Page 23 of 31
January performance was based on 3 breaches for the following reasons/areas:
• 1 x local surgery delay (Urology pathway) • 1 x tertiary oncology delay (LGI pathway) • 1 x external communication delay from Breast Test Wales (BTW)
Financial Update The Oncology & Cancer Services Directorate is marginally under spent by £0.002m. Previous sickness rates reported of 2.29% have deteriorated to 4.90% this month and as a result, the 4.79% target has not been achieved. There is approximately 1 WTE vacancy. HDUHB Financial Performance (see Integrated Performance Assurance Report: hyperlink page 3 – Our Staff and Resources Domain) The financial position at the end of February 2017 is £49.394m deficit. The Health Board’s 2016/17 draft Interim Integrated Medium Term Plan (IMTP) forecast a full year deficit of £38.3m or £35.1m year to date. The Health Board’s position has exceeded this forecast all year, mainly due to higher variable pay resulting from delay in recruitment, compared with planning assumptions, and to a much lesser extent increased costs in Continuing Health Care and Secondary Care drugs. At the September 2016 Board, the forecast deficit in 2016/17 was increased to £43.051m and was subject to funding support requested from Welsh Government of £4.5m for Welsh Government Delivery and Outcomes Framework/RTT and £2.5m for Winter Pressures. These allocations were received in month 9 totalling £6.31m. The revised forecast £43.051m was also subject to the delivery of savings through to the end of the year, representing a real change to the run rate (i.e. cash saving) through actions on variable pay, non pay and other opportunities. The actual performance at month 8 showed that the challenge in variable pay control was proving impossible. Additionally, pressures in non pay, Welsh Health Specialised Services Committee (WHSSC) and Primary Care prescribing, required the Health Board to restate the year end forecast

Page 24 of 31
deficit to £51.815m. The Health Board implemented the Handling Plan in month 9 and remains on track to deliver the revised deficit. The plan was dependent on a step up in savings totalling £2.8m in the final quarter, of which £1.7m was deemed higher risk, as it related mainly to variable pay savings. In month 10, in line with discussions with the Finance Director, Health and Social Services Group on the 8th February 2017, the Health Board reviewed the likely spend on the New Treatment Fund before year end. It is expected to be significantly less than the funding approved, therefore, following discussions with Board Colleagues, it was agreed to reduce the Forecast Deficit by the full allocation anticipated of £1.9m to £49.915m. The Health Board will look to mitigate the impact of new drug costs in 2016/17. The month 11 reports indicate that the Health Board should be able to manage these risks to year end. As was the case in 2015/16, the £7.475m, 2014/15 & £31.199m, 2015/16 deficit repayment has not been reflected, pending agreement with Welsh Government on the impact and timing of this on the remaining year of the 3 year rolling breakeven duty. In governance terms, the Board is now under ‘Targeted Intervention’. In summary, the February 2017 financial position is as follows:
Pay and non-pay continue to show cost pressures. The total pay bill in month 11 has decreased since month 10. The graph below shows the relationship between substantive and variable pay for the whole organisation since 2013/14. The trend lines show a static position in substantive pay, after accounting for pay awards, more than outweighed by an increase in variable pay (classified as agency, locum, bank and overtime) giving an overall increase as follows:
Summary Financial Position To date
AnnualPlan£m
Year to DatePlan£m
Year to DateActual
£m
Adverse/ (Positive) Variance
£m
Annual Plan Forecast Variance
£m
IncomeMiscellaneous Income (48.036) (44.354) (45.140) (0.786) 0.000Revenue Resource Limit (760.365) (689.576) (689.572) 0.004 0.000Non Resource Limited Income 1.060 1.035 1.035 0.000 0.000Total Income (807.341) (732.895) (733.677) (0.782) 0.000
ExpenditureLHB Provided Services - Pay 364.215 333.855 346.387 12.532 0.000LHB Provided Services - Non Pay 112.986 104.530 109.733 5.203 0.000Primary Care Prescribed Drugs & Appliances 68.927 63.183 63.474 0.291 0.000Primary Care Services 107.891 99.651 98.219 (1.432) 0.000Healthcare & Non Healthcare Services Provided By Other NHS Bodies including Specialised Services 124.771 114.405 114.876 0.471 0.000Private & Voluntary Sector 50.757 46.426 47.397 0.971 0.000Joint Financing & Other 4.244 3.958 2.985 (0.973) 0.000Other (mainly reserves) 11.850 1.995 0.000 (1.995) 0.000IMTP Deficit (38.300) (35.108) 0.000 35.108 38.300Financial Handling Plan Adjustments to Deficit Forecast 4.751Revised Assessment of Forecast 6.864
Total Expenditure 807.341 732.896 783.071 50.176 49.915
Total Deficit 0.000 0.001 49.395 49.394 49.915

Page 25 of 31
Compared with substantive budget which includes vacancies, the impact of variable pay in Planned and Unscheduled Care alone i.e. the premium costs being incurred above budget, is as follows:
The breakdown of variable pay costs over the same period by category is summarised in the following table. On average in 2015/16, the Health Board spent almost 3 times a month more than the 2013/14 position. This was the key driver of the deficit in 2015/16 and one of the Health Board’s highest priorities to address in 2016/17.
Month 12 2015/16 saw variable pay at £5.203m. This has been improved upon in 2016/17 (with the exception of month 6), but to reach the savings target, the Health Board is aiming to return to 2014/15 values as a first step. The Health Board is therefore not able to report any variable pay savings, although any reduction will contribute positively to the run-rate.
As noted above, the total pay bill in month 11 has decreased since month 10. This is due in the main to a decrease in the variable pay bill, with substantive pay remaining broadly similar in overall terms to the previous month. The biggest decrease was seen in registered nursing variable pay; split almost evenly between Unscheduled and Planned Care. Whilst this is welcome, the Health Board is treating this with caution at this time, as February is a shorter month and may be skewing the figures.
-
1,000
2,000
3,000
4,000
5,000
6,000
21,000
23,000
25,000
27,000
29,000
31,000
33,000
35,000
Varia
ble
Pay
£'00
0
Subs
tant
ive &
Tot
al Pa
y £'
000
Substantive pay Total Pay Variable pay Linear (Substantive pay) Linear (Total Pay) Linear (Variable pay)
Level 4 Location BUD WTE ACT WTE CUM BUD £ CUM EXP £ CUM VAR £ L4: PLANNED CARE BGH 253.51 216.27 11,881,309 13,049,749 1,168,440
GGH 580.20 563.92 26,039,608 28,985,067 2,945,459GGH/PPH 161.30 150.45 10,024,500 10,465,047 440,547No specific location identified 88.38 94.60 3,505,431 3,404,275 -101,157PPH 169.03 166.38 5,934,760 5,854,084 -80,676WGH 403.90 363.05 17,668,803 19,667,056 1,998,253
L4: PLANNED CARE Total 1,656.32 1,554.67 75,054,411 81,425,277 6,370,866L4: UNSCHEDULED CARE BGH 274.05 247.90 11,750,473 14,061,857 2,311,384
GGH 539.21 510.17 22,563,290 25,812,900 3,249,610PPH 364.53 391.66 14,821,418 18,180,058 3,358,640WGH 367.81 368.00 16,362,457 19,458,001 3,095,544PATHOLOGY 230.16 221.22 9,903,447 9,552,515 -350,932RADIOLOGY 211.68 199.77 10,410,139 11,372,393 962,254
L4: UNSCHEDULED CARE TOTAL 1,987.44 1,938.72 85,811,224 98,437,724 12,626,500Grand Total 3,643.76 3,493.39 160,865,635 179,863,001 18,997,366

Page 26 of 31
Figures for this month are as follows:
The IMTP sets out the ambition to deliver £29.4m of savings for 2016/17. The Health Board has developed a Quality Innovation Productivity and Prudency (QIPP) programme, focusing equally on service improvement as well as reducing cost. With this in mind, ten work-streams have been agreed, based on information gathered from benchmarking with others, to identify where the Health Board needs to tackle variation. There is also a general 1% cost improvement target. Unfortunately, as part of the review process at the end of the first quarter, the Health Board concluded that some of the work-streams will not deliver to the full amount anticipated in the IMTP in year. Focus to ensure progress is made between now and year end and development of schemes in readiness for 2017/18 is already in train. For the current year, the Health Board identified alternative funding streams / flexibility in reserves to compensate for 2016/17 non-delivery of savings plans. Having reviewed the position in month 10, the Executive Team has concluded that the forecast deficit should be restated at £49.915m. In reaching this figure, a risk assessment of savings delivery has been taken into account. Therefore against the original savings target of £29.4m, the Health Board is now forecasting delivery of £9.149m, together with previously identified release of reserves of £11.142m. The resultant shortfall combined with other cost pressures, offset by further compensating actions, contribute to the restated deficit of £49.915m. Gross savings delivery to month 11 is £8.061m, and combined with the alternative funding releases of £5.662m, brings this to £13.723m against a profile of £26.552m. Although the savings plans may not be delivering, the Health Board Handling Plan was dependent on a real reduction in the run rate of £1.5m for Variable pay, £1m in Continuing Health Care (CHC) and £0.3m for Non-Pay in the last quarter to achieve the revised forecast outturn. The Health Board has reviewed the risk associated with each of these areas. Variable pay remains high risk but there has been an improvement with the risk for CHC and Non-pay reducing, with the total risk now standing at £0.95m, which is anticipated to be managed.
2013/14 2014/15 2015/16 2016/17 2016/17 2016/17 % Variance ofAverage
Monthly CostAverage Monthly
Cost
Average Monthly Cost
Average Monthly Cost
to Date
Current Month Cost
Cumulative Cost to Date
Avge Monthly 15/16 vs Current Month
16/17£ £ £ £ £ £
AGENCY & PREMIUM COST LOCUM :
NURSING & MIDWIFERY REGISTERED 102,201 273,152 940,537 1,471,460 1,588,821 16,186,059 69%MEDICAL & DENTAL 233,785 157,729 127,327 162,999 204,169 1,792,989 60%PREMIUM COST LOCUM 0 368,529 642,492 1,084,155 1,054,991 11,925,706 64%ADDITIONAL CLINICAL SERVICES NURSING ASSISTANTS 4,315 24,927 165,189 238,786 181,273 2,626,644 10% OTHER ACS STAFF 1,097 1,424 1,343 1,512 -3,137 16,631 -334%ADDITIONAL CLINICAL SERVICES TOTAL 5,412 26,351 166,532 240,298 178,135 2,643,276 7%ADD PROF SCIENTIFIC & TECHNICAL 492 3,258 26,408 19,062 4,013 209,680 -85%ADMINISTRATIVE & CLERICAL -5 176 7,339 31,832 18,374 350,153 150%ALLIED HEALTH PROFESSIONALS 0 164 20,863 159,350 157,793 1,752,849 656%ESTATES & ANCILLIARY 0 2,582 131 3,881 -778 42,688 -696%HEALTHCARE SCIENTISTS 6,721 4,601 22,890 56,882 63,898 625,698 179%AGENCY/PREMIUM COST LOCUM TOTAL 348,606 836,542 1,954,518 3,229,918 3,269,416 35,529,099 67%
MEDICAL LOCUM 255,421 292,205 512,783 526,704 513,656 5,793,740 0%
BANK NURSING & MIDWIFERY REGISTERED 226,475 239,590 229,263 212,225 159,221 2,334,475 -31% NURSING ASSISTANTS 237,469 285,900 310,022 412,128 416,468 4,533,403 34%
BANK TOTAL 463,944 525,490 539,285 624,353 575,690 6,867,878 7%
OVERTIME 127,258 190,305 253,503 337,599 317,270 3,713,587 25%
TOTAL 1,195,230 1,844,542 3,260,088 4,718,573 4,676,032 51,904,303 43%

Page 27 of 31
HDUHB Workforce (see Integrated Performance Assurance Report: hyperlink page 3 – Our Staff and Resources Domain) Sick Absence The rolling sickness information was as 5.2% as at 31st January 2017, which is a 0.38% reduction against the January 2016 position. The in month actual figure reported for January equates to 5.70% which disappointingly represents an increase of 0.43% against the previous month (December 2016) although still represents a slight improvement of 0.03% against the corresponding period last year i.e. January 2016. Recruitment The Health Board attended Swansea University 3rd Year Student Open Day on 3rd February. A Newly Qualified (NQ) 2017 advert followed which ran for 10 days, accompanied by a social media campaign. Further applicants ranged from Bangor, Bristol, Cardiff and Swansea. HDUHB Twitter account went live (English and Welsh) on 28th February to compliment and promote all campaign activity. A refreshed approach to LinkedIn has resulted in ongoing enquiries, including a GMC registered Radiologist from Serbia, ENT Surgeon from Istanbul and a Flight Doctor at Capital Air Ambulance from Somerset. Skype interviews have been arranged. Occupational Therapy (OT) and Physiotherapy Showcase pages have gone live on LinkedIn in support of ongoing campaigns to recruit. Two OT’s have approached the Campaigns team in response to a targeted University poster. Pembrokeshire College have started filming for OT and Physiotherapy Campaigns. The London Underground advert went live on 13th February. Enquiries have been received to date from a Junior Doctor, Band 7 Theatre Practitioner, Midwife, 2 Physiotherapists and an OT. A Recruitment Open Day will take place in September 2017 for GGH to capture the holiday makers during the advertising campaign. The Paediatric recruitment campaign went live on Monday 6th March, supported by advertising, testimonials and professionally produced videos. International Recruitment Five Philippine nurses have arrived in Wales, 3 have commenced their orientation. 9 Italian nurses sat their International English Language Testing System (IELTS) exam, but regrettably 8 failed the exam, and one passed her IELTS on her first attempt. This individual will now apply for registration with the Nursing and Midwifery Council (NMC). Medical Recruitment Consultant Appointments – Health Board Wide Name Department & Base Dr Annette Edwards Consultant in Palliative Medicine
Base: WGH Start Date: 6th February 2017
Dr Saba Kebede
Consultant Acute Physician Base: GGH Start Date: 1st March 2017
Mr Tom Betts
Consultant Ophthalmologist Base: GGH Start Date: July 2018 (working 1 session per week from April 2017)
Mr Sam Evans
Consultant Ophthalmologist Base: GGH

Page 28 of 31
Start Date: will undertake sessions before commencing Full time on 4th September 2017
Ms Guzaliya Safiullina
Consultant Ophthalmologist Base: BGH Start Date: 3rd June 2017
Mr Vummiti Muralikrishnan
Consultant Breast Surgeon Base: PPH Start Date: 1st June 2017
Dr Mark Andrews Consultant in Respiratory Medicine Base: PPH Start Date: 1st August 2017 (TBC)
Locum Consultants Department & Base: Dr Kasturibai Dharman
Locum Consultant Radiologist (Working towards CESR for Substantive post) Base: GGH Commencing Feb 2017
Dr Ravi Kakkar
Locum Consultant General Paediatrician Base : WGH Commencing: 6th March 2017
Dr Talar Abdul-Rahman Amin
Locum Consultant in Obstetrics & Gynaecology Base: WGH Commencing: 1st March 2017
Dr Matouk Zbaeda
Locum Consultant Paediatrician (will be asked to apply for substantive post if they like the area) Base: GGH Commencing: 3rd April 2017 (TBC)
Dr Huda Sadek
Locum Consultant Community Paediatrician (will be asked to apply for substantive if they like the area) Base: Llanelli Commencing : 5th June 2017 (TBC)
A further 12 Consultant level doctors have been appointed in February 2017 (7 substantive appointments and 5 Locum Consultant appointments) totalling 18 appointments for the first 2 months of the year. Further Advanced Applications Consultant (AAC) interviews are scheduled in March 2017.
The Health Board is also continuing to source Locum doctors from permanent recruitment agencies, paying a finders fee and 2 Paediatricians and a Radiologist have been secured.
Middle/Junior Grade Medical posts The Health Board appointed 14 middle and junior posts across the Health Board during February. In addition, 6 previously appointed middle and junior posts started in February. Bank Bank recruitment continues. Twenty four Healthcare Support Workers (HCSW) for learning disabilities were interviewed on 28th February. Forty eight student nurses have applied for Bank HCSW posts. Nine Registered Nurses (RN’s) have been shortlisted and will be interviewed on March 2nd. There are 87 applicants for this month’s mental health advert for short listing. Registered Nursing recruitment remains a challenge but 9 applicants for the March interviews are positive.

Page 29 of 31
Mandatory Training The current figures represent a significant overall improvement of 10.2% taking the UHB above 50% compliance, with improvement percentage increase between 1.5% and 2.7% in all areas. The improvement is likely to be in part a reflection of the manually loaded e-learning. There has been an improvement in the 12 month period from 42% in February 2016 to 50.4% February 2017. The previously reported issue in terms of the reporting of e-learning due to the change from Oracle Learning Management to the new Electronic Staff Record (ESR) Learning Management System platform in January has been resolved. The ESR system is currently being further refined to simplify access for users and this is being piloted/tested in Velindre NHS Trust to identify and manage any operational issues before roll out across NHS Wales. PADR (Performance Appraisal Development Review) Medical Staff Appraisal continues to be on target at 92% which is above the target of 85% and represents a 1% improvement from January 2017. The Health Board overall compliance rate for non-medical PADR’s is 51.29%. This represents an increase overall in month of 0.8% against the 85% target. Twelve areas have shown an improvement on the January 2016 position, with 14 areas showing a decrease, 6 of these with a decrease of less than 1%. Unscheduled Care in PPH is showing the greatest increase in month of 5.07% with improvement from 51.59% in February 2016 to 67.38% in February 2017. Other Live Issues Corporate Health Standard The full assessment for the Gold standard for our Corporate Health Standard Accreditation took place on the 8th and 9th February 2017. Three external assessors reviewed the action plan criteria completed by Organisational Development Department. The assessors also visited three acute and two community sites to speak to staff regarding Health and Well Being initiatives in Hywel Dda. Feedback was very positive and our department awaits the assessor’s formal report. Platinum assessment will now take place on 22nd March 2017. Work Experience The Organisational Development team are currently in discussions with Workforce, Education and Development Services (WEDS) regarding becoming an exemplar for Work Experience. This involves building on the excellent progress made in this service with the new and exciting programmes added last year. The Health Board is hopeful that this experience will lead individuals into a career in health care whilst removing the negative perceptions of work experience. Values The implementation of the values is now complete but there is now the challenge to get them embedded. The Organisational Development (OD) team are reviewing various means of getting the values incorporated into policies and processes. There are also discussions in relation to how to start building psychological safety within the organisation, so employees are comfortable in challenging poor behaviours. The Twitter feed is live but very slow in getting people to tag it into areas where the values are being demonstrated. The chairs employee/team, of the month has had a new values incorporated nomination form and certificate uploaded onto the staff intranet. This will ensure that staff are being recognised for the values/behaviours they demonstrate as part of the award nomination.

Page 30 of 31
Exit Interviews A new exit interview has now been launched and is available online on the forms library and values ages. There are a number of ways a leaver can complete the questionnaire. Ideally the questionnaire should be completed with their line manager. However, the Health Board recognises that some staff would not wish to do this. Therefore, alternatives are available including another manager, Human Resources, OD, or on-line. The Health Board also wishes to capture experiences of staff moving from one department to another. It is hoped that that through these different options, an increase in the response rate will be seen. The new questionnaire has been designed to measure the values and health and wellbeing as well as reasons for leaving. Welsh Language The Health Board is second highest in NHS Health Boards in Wales, second only to the Welsh Ambulance Service in terms of accurately recording the Welsh Language competency of our staff with ESR, reflecting information on 71% of our workforce. The Workforce and OD team are currently working with the Welsh Language officers to evaluate the impact of the anticipated implications of the revised Welsh Language Standards, and identify actions locally and those better placed to be managed nationally. The UHB was very pleased to note that the results of the Staff Survey reflected that 66% of the respondents from the UHB stated ‘that the team I work in is able to provide services in Welsh when this is the preference of the service user’ which was 18% higher than the NHS Wales average. Argymhelliad / Recommendation The Board is requested to discuss the report and to raise any issues arising from the content.
Amcanion: (rhaid cwblhau) Objectives: (must be completed) Safon(au) Gofal ac Iechyd: Health and Care Standard(s):
Amcanion Strategol y BI: HB Strategic Objectives:
IMTP 2015-2018
Gwybodaeth Ychwanegol: Further Information: Ar sail tystiolaeth: Evidence Base:
NHS Outcome Framework and measures guidance 2016-17 WHC (2016) 023
Rhestr Termau: Glossary of Terms:
WG – Welsh Government IMTP – Integrated Medium Term Plan USC – Urgent Suspected Cancer RTT – Referral to Treatment DNA – Did not Attend A&E – Accident & Emergency IPFR – Individual Patient Funding Request WHSSC – Welsh Health Specialised Services Committee NICE – National Institute for Health and Care Excellence AWMSG – All Wales Medicines Strategy Group

Page 31 of 31
AWTTC - All Wales Therapeutic and Toxicology Centre INNU – Interventions Not Normally Undertaken EqIA - Equality Impact Assessment
Partïon / Pwyllgorau â ymgynhorwyd ymlaen llaw y Cyfarfod Bwrdd Iechyd Prifysgol: Parties / Committees consulted prior to University Health Board Meeting:
Finance, Performance, Quality and Safety, Nursing, Information, Workforce, Mental Health, Primary Care
Effaith: (rhaid cwblhau) Impact: (must be completed) Ariannol / Gwerth am Arian: Financial / VFM:
Better use of resources through integration of reporting methodology
Risg / Cyfreithiol: Risk / Legal:
Better use of resources through integration of reporting methodology
Answadd / Gofal Claf: Quality / Patient Care:
Use of key metrics to triangulate and analyse data to support improvement
Gweithlu: Workforce:
Development of staff through pooling of skills and integration of knowledge
Cydraddoldeb: Equality:
• Has EqIA Screening been undertaken? Not applicable • Has a full EqIA been undertaken? Not applicable